Anda mungkin juga menyukai
- Paper No.2 ModifiedDokumen6 halamanPaper No.2 ModifiedAndrew Surya Putra SccBelum ada peringkat
- 608751Dokumen8 halaman608751adesamboraBelum ada peringkat
- Effect of Coffe & Stress With The Incidedence of GastritisDokumen5 halamanEffect of Coffe & Stress With The Incidedence of GastritisJufran, R (2018)Belum ada peringkat
- THE Canadian Medical Association: Associate, Department of Dermatology, Vancouver General Hospital, Vancouver, B.CDokumen5 halamanTHE Canadian Medical Association: Associate, Department of Dermatology, Vancouver General Hospital, Vancouver, B.CAndrew Surya Putra SccBelum ada peringkat
- 608751Dokumen8 halaman608751adesamboraBelum ada peringkat
- THE Canadian Medical Association: Associate, Department of Dermatology, Vancouver General Hospital, Vancouver, B.CDokumen5 halamanTHE Canadian Medical Association: Associate, Department of Dermatology, Vancouver General Hospital, Vancouver, B.CAndrew Surya Putra SccBelum ada peringkat
- Psoriasis Treated Acetonii) E AND Occlusive Dressings: With Topical FluocinoloneDokumen2 halamanPsoriasis Treated Acetonii) E AND Occlusive Dressings: With Topical FluocinoloneAndrew Surya Putra SccBelum ada peringkat
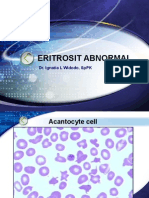
- Eritrosit AbnormalDokumen20 halamanEritrosit AbnormalAndrew Surya Putra SccBelum ada peringkat
- Dkamanagment 150323150043 Conversion Gate01Dokumen28 halamanDkamanagment 150323150043 Conversion Gate01Andrew Surya Putra SccBelum ada peringkat
- Dka Pathphysiologymanagement2014 Copy 140202235658 Phpapp02Dokumen31 halamanDka Pathphysiologymanagement2014 Copy 140202235658 Phpapp02Andrew Surya Putra SccBelum ada peringkat
- Eritrosit Hipokrom Mikrositer, Pencil CellDokumen6 halamanEritrosit Hipokrom Mikrositer, Pencil CellAndrew Surya Putra SccBelum ada peringkat
- Slide UrineDokumen15 halamanSlide UrineAndrew Surya Putra SccBelum ada peringkat
- Dka Pathphysiologymanagement2014 Copy 140202235658 Phpapp02Dokumen31 halamanDka Pathphysiologymanagement2014 Copy 140202235658 Phpapp02Andrew Surya Putra SccBelum ada peringkat
- DKADokumen12 halamanDKAAisha SyedBelum ada peringkat
- CVM 00288tDokumen6 halamanCVM 00288tAndrew Surya Putra SccBelum ada peringkat
- Afib Info SheetDokumen2 halamanAfib Info Sheetapi-265745737Belum ada peringkat
- Diabetic Ketoacidosis: Abdelaziz Elamin Professor of Pediatric Endocrinology University of Khartoum, SudanDokumen33 halamanDiabetic Ketoacidosis: Abdelaziz Elamin Professor of Pediatric Endocrinology University of Khartoum, SudanboyzbanjarboyzBelum ada peringkat
- DkaDokumen23 halamanDkaAnissa tri acintyaBelum ada peringkat
- Presented by DR Ashish Sharma Guided by DR Meena PatelDokumen74 halamanPresented by DR Ashish Sharma Guided by DR Meena PatelAndrew Surya Putra SccBelum ada peringkat
- Bab 8 Daftar PustakaDokumen10 halamanBab 8 Daftar PustakaAndrew Surya Putra SccBelum ada peringkat
- ReferenceDokumen8 halamanReferenceAndrew Surya Putra SccBelum ada peringkat
- CVM 00288tDokumen6 halamanCVM 00288tAndrew Surya Putra SccBelum ada peringkat
- CVM 00288tDokumen6 halamanCVM 00288tAndrew Surya Putra SccBelum ada peringkat
- Bab 8 Daftar PustakaDokumen10 halamanBab 8 Daftar PustakaAndrew Surya Putra SccBelum ada peringkat
- 0065Dokumen4 halaman0065Andrew Surya Putra SccBelum ada peringkat
- Pathophysiology of Atrial FibrillationDokumen12 halamanPathophysiology of Atrial FibrillationAndrew Surya Putra SccBelum ada peringkat
- ORBIT Guidelines Poster AHA v2-EmilyOBrien-SUNDAY - 9amDokumen1 halamanORBIT Guidelines Poster AHA v2-EmilyOBrien-SUNDAY - 9amAndrew Surya Putra SccBelum ada peringkat
- Atrial Fibrillation: The Management of Atrial Fibrillation: Issued: June 2014 Last Modified: August 2014Dokumen50 halamanAtrial Fibrillation: The Management of Atrial Fibrillation: Issued: June 2014 Last Modified: August 2014Andrew Surya Putra SccBelum ada peringkat
- Topical Cyclosporine in The Treatment of Allergic ConjunctivitisDokumen7 halamanTopical Cyclosporine in The Treatment of Allergic ConjunctivitisRandy AninditoBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Thesis Committee MeetingDokumen7 halamanThesis Committee Meetingafknojbcf100% (2)
- Dopamine What It Is, Function & SymptomsDokumen7 halamanDopamine What It Is, Function & SymptomsRaj KumarBelum ada peringkat
- BSCHMCTT 101Dokumen308 halamanBSCHMCTT 101JITTUBelum ada peringkat
- Ministry of Truth Big Brother Watch 290123Dokumen106 halamanMinistry of Truth Big Brother Watch 290123Valentin ChirilaBelum ada peringkat
- Summarized ACLS ScriptDokumen7 halamanSummarized ACLS Scriptnc.angel.niceBelum ada peringkat
- Parwati DeviDokumen25 halamanParwati DevikvntpcsktprBelum ada peringkat
- Tugas, MO - REVIEW JURNAL JIT - Ikomang Aditya Prawira Nugraha (1902612010304)Dokumen12 halamanTugas, MO - REVIEW JURNAL JIT - Ikomang Aditya Prawira Nugraha (1902612010304)MamanxBelum ada peringkat
- FreeMarkets: Procurement & Outsourcing StrategiesDokumen44 halamanFreeMarkets: Procurement & Outsourcing StrategiesFarhaad MohsinBelum ada peringkat
- LET Facilitating Learning EDITED3Dokumen12 halamanLET Facilitating Learning EDITED3Likhaan PerformingArts HomeStudio100% (5)
- Malefactor ClassDokumen23 halamanMalefactor ClassMatthew Duncan100% (6)
- Commercial CrimesDokumen3 halamanCommercial CrimesHo Wen HuiBelum ada peringkat
- Donor S Tax Exam AnswersDokumen6 halamanDonor S Tax Exam AnswersAngela Miles DizonBelum ada peringkat
- International Conference On Basic Science (ICBS)Dokumen22 halamanInternational Conference On Basic Science (ICBS)repositoryIPBBelum ada peringkat
- Scipaper 7Dokumen2 halamanScipaper 7JL Serioso BalesBelum ada peringkat
- Brain Imaging TechniquesDokumen6 halamanBrain Imaging TechniquesIlika Guha MajumdarBelum ada peringkat
- Csm6 Ext1y11 BookDokumen955 halamanCsm6 Ext1y11 BookJesse Davis100% (12)
- The Bible Does Not Condemn Premarital SexDokumen16 halamanThe Bible Does Not Condemn Premarital SexKeith502100% (3)
- Week9 Phylum NemathelminthesDokumen26 halamanWeek9 Phylum NemathelminthesCzerinne Angela Justinne AlarillaBelum ada peringkat
- Asset Management PlanDokumen160 halamanAsset Management Planbkalatus1100% (1)
- RegressionDokumen16 halamanRegressionchinusccBelum ada peringkat
- Institute of Actuaries of India: Subject CT3-Probability and Mathematical Statistics May 2008 ExaminationDokumen10 halamanInstitute of Actuaries of India: Subject CT3-Probability and Mathematical Statistics May 2008 ExaminationeuticusBelum ada peringkat
- Attery: User Guide Dict Release 2020Dokumen47 halamanAttery: User Guide Dict Release 2020diegoBelum ada peringkat
- LakmeDokumen34 halamanLakmeSuraj Pratap Sawhney79% (14)
- Jesus Christ Was A HinduDokumen168 halamanJesus Christ Was A Hinduhbk22198783% (12)
- Aìgas of Bhakti. at The End of The Last Chapter Uddhava Inquired AboutDokumen28 halamanAìgas of Bhakti. at The End of The Last Chapter Uddhava Inquired AboutDāmodar DasBelum ada peringkat
- A Scenario of Cross-Cultural CommunicationDokumen6 halamanA Scenario of Cross-Cultural CommunicationN Karina HakmanBelum ada peringkat
- Sri Guru Parampara Stotram CompressDokumen14 halamanSri Guru Parampara Stotram CompressSatishPavurayalaBelum ada peringkat
- Sale Deed Document Rajyalakshmi, 2222222Dokumen3 halamanSale Deed Document Rajyalakshmi, 2222222Madhav Reddy100% (2)
- Measure For Measure AngeloDokumen1 halamanMeasure For Measure AngeloRoger Knight100% (1)
- Improving Self-Esteem - 08 - Developing Balanced Core BeliefsDokumen12 halamanImproving Self-Esteem - 08 - Developing Balanced Core BeliefsJag KaleyBelum ada peringkat