Anda mungkin juga menyukai
- Chest Trauma ManagementDokumen78 halamanChest Trauma ManagementHassan Shoukat100% (1)
- Intercostal DrainDokumen44 halamanIntercostal Drainvamshidh100% (1)
- Internal MedicineDokumen167 halamanInternal MedicineJason Steel86% (7)
- 5-Thoracic Surgery PT &ot 2023-2024-1Dokumen114 halaman5-Thoracic Surgery PT &ot 2023-2024-1MUGISHA GratienBelum ada peringkat
- Chest Injuries: DR Rodwell Gundo Medical/Surgical Nursing DepartmentDokumen47 halamanChest Injuries: DR Rodwell Gundo Medical/Surgical Nursing Departmentpaul kaundaBelum ada peringkat
- Chest TraumaDokumen115 halamanChest TraumaЕвгений ХанькоBelum ada peringkat
- Chest Trauma DikaDokumen46 halamanChest Trauma DikaOnyedika EgbujoBelum ada peringkat
- Chest TraumaDokumen39 halamanChest Traumayared getachewBelum ada peringkat
- Chest TraumaDokumen35 halamanChest Traumaabu saniBelum ada peringkat
- Thoracic and Abdominal TraumaDokumen39 halamanThoracic and Abdominal TraumaIlliati IbrahimBelum ada peringkat
- Thorax TraumaDokumen24 halamanThorax TraumauffaanBelum ada peringkat
- Breathing and Ventilation EmergenciesDokumen13 halamanBreathing and Ventilation EmergenciesgosegomangBelum ada peringkat
- PneumothoraxDokumen30 halamanPneumothoraxsanjivdas100% (1)
- Chest Trauma: - Presented By: - November 19, 2012Dokumen137 halamanChest Trauma: - Presented By: - November 19, 2012Manuela CormioBelum ada peringkat
- Chest Trauma BCECDokumen25 halamanChest Trauma BCECTandin SonamBelum ada peringkat
- Torso TraumaDokumen37 halamanTorso TraumaFiza MushtaqBelum ada peringkat
- ChesttubesDokumen30 halamanChesttubesapi-2692977900% (1)
- AirwayDokumen15 halamanAirwayYonathan asnakeBelum ada peringkat
- 1 - PPT DR Taufik Nur Yahya SPBTKVDokumen46 halaman1 - PPT DR Taufik Nur Yahya SPBTKVAmry YusufBelum ada peringkat
- NursingBulletin Notes On PneumothoraxDokumen27 halamanNursingBulletin Notes On Pneumothoraxseigelystic100% (11)
- Chest Injury and Its TypesDokumen14 halamanChest Injury and Its TypesKoochi PoojithaBelum ada peringkat
- Chest TraumaDokumen23 halamanChest TraumaMutaz DredeiBelum ada peringkat
- Day 1 - APPEC 2021Dokumen492 halamanDay 1 - APPEC 2021GaurieBelum ada peringkat
- HematotoraksDokumen15 halamanHematotorakssafanj12Belum ada peringkat
- RLS Chest TraumaDokumen31 halamanRLS Chest TraumaSanthu MeprathuBelum ada peringkat
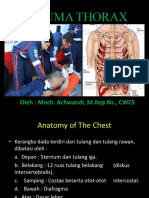
- Trauma Thorax: Oleh: Moch. Achwandi, M.Kep - NS., CWCSDokumen51 halamanTrauma Thorax: Oleh: Moch. Achwandi, M.Kep - NS., CWCSMas sobah SobahBelum ada peringkat
- Chest Trauma: Nursing 410 Western Carolina University BSN ProgramDokumen29 halamanChest Trauma: Nursing 410 Western Carolina University BSN ProgramShimmering MoonBelum ada peringkat
- Water Sael DrainageDokumen36 halamanWater Sael DrainageerlinaBelum ada peringkat
- Lower Resp TraumaDokumen62 halamanLower Resp TraumaA Rezki ChairamsyahBelum ada peringkat
- Chest TraumaDokumen31 halamanChest Traumawheeyycoldandhot55Belum ada peringkat
- Trauma Thorax: Oleh: Moch. Achwandi, M.Kep - NS., CWCSDokumen52 halamanTrauma Thorax: Oleh: Moch. Achwandi, M.Kep - NS., CWCSMariSstan EM HaBelum ada peringkat
- Disorders of The PleuraDokumen31 halamanDisorders of The PleuraKathleen Dela CruzBelum ada peringkat
- Chest Tubes and Drainage Systems: Deb Updegraff RN, CNS Picu LPCHDokumen28 halamanChest Tubes and Drainage Systems: Deb Updegraff RN, CNS Picu LPCHLucila LugoBelum ada peringkat
- Nursing Care of Patients With Pneumothorax: Prepared By: N. WadeDokumen33 halamanNursing Care of Patients With Pneumothorax: Prepared By: N. WadeokaciaBelum ada peringkat
- Chapter 3Dokumen54 halamanChapter 3Ayro Business CenterBelum ada peringkat
- Pneumothorax AmierDokumen7 halamanPneumothorax Amieramier90Belum ada peringkat
- Spontaneous Pneumothorax For General Surgical Residents: Facebook: Happy Friday Knight January, 12, 2018 ThailandDokumen64 halamanSpontaneous Pneumothorax For General Surgical Residents: Facebook: Happy Friday Knight January, 12, 2018 ThailandGrace SomsirivattanaBelum ada peringkat
- Pemicu 2 KGD AditDokumen80 halamanPemicu 2 KGD AditAditya SuksmawanBelum ada peringkat
- Trauma Thoraks PDFDokumen86 halamanTrauma Thoraks PDFMiftahurrahmiBelum ada peringkat
- Chest TraumaDokumen62 halamanChest TraumaayouBelum ada peringkat
- ICDDokumen36 halamanICDAnusha Verghese100% (1)
- Traumatic Chest InjuryDokumen26 halamanTraumatic Chest InjurySarahBelum ada peringkat
- 4954thoracic TraumaDokumen43 halaman4954thoracic TraumaSahilSharmaBelum ada peringkat
- Injuries To The Chest Wall Lungop InkejuryDokumen88 halamanInjuries To The Chest Wall Lungop InkejuryNudžejma KadrićBelum ada peringkat
- Chest Trauma: CDR John P Wei, Usn MC MD 4 Medical Battallion, 4 MLG BSRF-12Dokumen38 halamanChest Trauma: CDR John P Wei, Usn MC MD 4 Medical Battallion, 4 MLG BSRF-12Cora TateBelum ada peringkat
- Thoracic Trauma - Navy - PSPD 2021Dokumen45 halamanThoracic Trauma - Navy - PSPD 2021Naavy LaksmonoBelum ada peringkat
- Chest TraumaDokumen44 halamanChest TraumaThein Mui KyunBelum ada peringkat
- Pneumothorax: - Hitesh Rohit (3 Year B.P.T.)Dokumen22 halamanPneumothorax: - Hitesh Rohit (3 Year B.P.T.)Hitesh RohitBelum ada peringkat
- Pneumothorax: - Hitesh Rohit (3 Year B.P.T.)Dokumen22 halamanPneumothorax: - Hitesh Rohit (3 Year B.P.T.)Hitesh RohitBelum ada peringkat
- Managing Chest DrainageDokumen63 halamanManaging Chest DrainagecarlalynneBelum ada peringkat
- Trauma Thorax: Oleh: Moch. Achwandi, M.Kep - NS., CWCSDokumen52 halamanTrauma Thorax: Oleh: Moch. Achwandi, M.Kep - NS., CWCSMariSstan EM HaBelum ada peringkat
- Asuhan Keperawatan Trauma Dada PDFDokumen67 halamanAsuhan Keperawatan Trauma Dada PDFbambang aryantoBelum ada peringkat
- Early Assessment of Trauma Patients and ATLSDokumen45 halamanEarly Assessment of Trauma Patients and ATLSTILAHUNBelum ada peringkat
- Chest Trauma and Thorocic InjuriesDokumen17 halamanChest Trauma and Thorocic Injuriespreet kaurBelum ada peringkat
- Chest TubesDokumen27 halamanChest TubesJerson EdilloBelum ada peringkat
- Thoracic Trauma ModifiedDokumen37 halamanThoracic Trauma ModifiedErfandiBelum ada peringkat
- Pneumothorax 1Dokumen53 halamanPneumothorax 1Tara BasnetBelum ada peringkat
- Tension Pneumothorax: Anak Agung Istri Intan YuniariDokumen19 halamanTension Pneumothorax: Anak Agung Istri Intan Yuniarifaris nagibBelum ada peringkat
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsDari EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsBelum ada peringkat
- INDIVIDUAL CASE ANALYSIS ScribdDokumen2 halamanINDIVIDUAL CASE ANALYSIS ScribdAnusha VergheseBelum ada peringkat
- Roy's Adaptation ModelDokumen2 halamanRoy's Adaptation ModelAnusha VergheseBelum ada peringkat
- Allergic Reactions: What To Look ForDokumen2 halamanAllergic Reactions: What To Look ForAnusha VergheseBelum ada peringkat
- Medical TerminologyDokumen2 halamanMedical TerminologyAnusha VergheseBelum ada peringkat
- Endotracheal IntubationDokumen1 halamanEndotracheal IntubationAnusha VergheseBelum ada peringkat
- TerminologyDokumen2 halamanTerminologyAnusha VergheseBelum ada peringkat
- SMART Learning Goals.Dokumen3 halamanSMART Learning Goals.Anusha VergheseBelum ada peringkat
- Bites and StingsDokumen1 halamanBites and StingsAnusha VergheseBelum ada peringkat
- Care Guidelines For Minor Open WoundsDokumen1 halamanCare Guidelines For Minor Open WoundsAnusha VergheseBelum ada peringkat
- Procedure Trays ListDokumen1 halamanProcedure Trays ListAnusha VergheseBelum ada peringkat
- ColicDokumen1 halamanColicAnusha VergheseBelum ada peringkat
- Chemical Burns First AidDokumen1 halamanChemical Burns First AidAnusha VergheseBelum ada peringkat
- Prevent Water Related InjuriesDokumen1 halamanPrevent Water Related InjuriesAnusha VergheseBelum ada peringkat
- Chest Xray InterpretationDokumen3 halamanChest Xray InterpretationAnusha VergheseBelum ada peringkat
- S.N o Criteria Yes No Remarks: Checklist For Intra-Hospital Transport of PatientDokumen2 halamanS.N o Criteria Yes No Remarks: Checklist For Intra-Hospital Transport of PatientAnusha VergheseBelum ada peringkat
- Gastric LavageDokumen2 halamanGastric LavageAnusha VergheseBelum ada peringkat
- Inducing Hypothermia in Post Cardiac Arrest PatientsDokumen2 halamanInducing Hypothermia in Post Cardiac Arrest PatientsAnusha VergheseBelum ada peringkat
- CholeraDokumen9 halamanCholeraAnusha VergheseBelum ada peringkat
- What Is Hodgkin's Disease?: Lymphoma CancerDokumen4 halamanWhat Is Hodgkin's Disease?: Lymphoma CancerAnusha VergheseBelum ada peringkat
- Protocol On Transcutaneous PacingDokumen7 halamanProtocol On Transcutaneous PacingAnusha VergheseBelum ada peringkat
- IV Lines and Safety Measures in Its Use For PatientsDokumen2 halamanIV Lines and Safety Measures in Its Use For PatientsAnusha VergheseBelum ada peringkat
- TB DiseaseDokumen3 halamanTB DiseaseAnusha VergheseBelum ada peringkat
- S.N o Criteria Yes No Remarks: Checklist For Intra-Hospital Transport of PatientDokumen2 halamanS.N o Criteria Yes No Remarks: Checklist For Intra-Hospital Transport of PatientAnusha VergheseBelum ada peringkat
- Infection and Its Mode of TransmissionDokumen33 halamanInfection and Its Mode of TransmissionAnusha Verghese100% (1)
- Multiple MyelomaDokumen10 halamanMultiple MyelomaFadina RizkiBelum ada peringkat
- Leukemia 5Dokumen26 halamanLeukemia 5Anusha VergheseBelum ada peringkat
- Leukemias Nursing ManagementDokumen20 halamanLeukemias Nursing ManagementAnusha Verghese100% (5)
- Blood TransfusionDokumen20 halamanBlood TransfusionAnusha VergheseBelum ada peringkat
- Lymphomas 5Dokumen32 halamanLymphomas 5Anusha VergheseBelum ada peringkat
- LeukemiasDokumen8 halamanLeukemiasAr-jay JubaneBelum ada peringkat
- Data Sheet Data Sheet: Gelafusal GelafusalDokumen2 halamanData Sheet Data Sheet: Gelafusal Gelafusalfahri azwarBelum ada peringkat
- Neem TreeDokumen4 halamanNeem Treedorzky22Belum ada peringkat
- Sexually Transmitted InfectionsDokumen18 halamanSexually Transmitted InfectionsEthan Matthew Hunt100% (1)
- Neuropsychologia: Jade Dignam, David Copland, Alicia Rawlings, Kate O 'Brien, Penni Burfein, Amy D. RodriguezDokumen12 halamanNeuropsychologia: Jade Dignam, David Copland, Alicia Rawlings, Kate O 'Brien, Penni Burfein, Amy D. RodriguezFrancisco Beltrán NavarroBelum ada peringkat
- EYE Emergency Manual An Illustrated Guide: Second EditionDokumen56 halamanEYE Emergency Manual An Illustrated Guide: Second Editionmanleyj5305Belum ada peringkat
- Unusual Interventions-3Dokumen113 halamanUnusual Interventions-3Vali Mariana Radulescu100% (2)
- Vadney Resume 2Dokumen2 halamanVadney Resume 2api-251597905Belum ada peringkat
- Computer Generated in Nursing Care PlansDokumen4 halamanComputer Generated in Nursing Care PlansCake Man100% (1)
- ResumeDokumen3 halamanResumeAstig Kuging63% (8)
- Vieillard-Baron2018 Article DiagnosticWorkupEtiologiesAndMDokumen17 halamanVieillard-Baron2018 Article DiagnosticWorkupEtiologiesAndMFranciscoBelum ada peringkat
- CarcinogenDokumen196 halamanCarcinogenJosé RamírezBelum ada peringkat
- How - . - I Train Others in Dysphagia.Dokumen5 halamanHow - . - I Train Others in Dysphagia.Speech & Language Therapy in PracticeBelum ada peringkat
- Survanta PiDokumen10 halamanSurvanta PiBas BaylonBelum ada peringkat
- Kevin Chen - Book Review: Scientific Qigong Exploration: The Wonders and Mysteries of Qi by Lu, ZuyinDokumen6 halamanKevin Chen - Book Review: Scientific Qigong Exploration: The Wonders and Mysteries of Qi by Lu, ZuyinSonyRedBelum ada peringkat
- Paul Holmes, Steve Farnfield - The Routledge Handbook of Attachment - Implications and Interventions-Routledge (2014)Dokumen205 halamanPaul Holmes, Steve Farnfield - The Routledge Handbook of Attachment - Implications and Interventions-Routledge (2014)Pamela Fontánez100% (4)
- Periodontal Infection Control: Current Clinical ConceptsDokumen10 halamanPeriodontal Infection Control: Current Clinical ConceptsNunoGonçalvesBelum ada peringkat
- Youstina Khalaf Exam 26-5Dokumen6 halamanYoustina Khalaf Exam 26-5M Usman KhanBelum ada peringkat
- Emotional IntelligenceDokumen19 halamanEmotional IntelligenceShweta ShrivastavaBelum ada peringkat
- 15.chronic - Venous - Insufficeincy (Sukrita 22.8.60)Dokumen17 halaman15.chronic - Venous - Insufficeincy (Sukrita 22.8.60)Juli VlogBelum ada peringkat
- Punjab Drugs Rules 2007Dokumen33 halamanPunjab Drugs Rules 2007RphNaeemMalik75% (12)
- HeatStress NEWDokumen33 halamanHeatStress NEWJeffrey Arandia100% (1)
- Plaque ControlDokumen52 halamanPlaque ControlIbrahim AbdelHadi100% (1)
- Diagnosis & Management of NstemiDokumen26 halamanDiagnosis & Management of NstemiwlshakespeareBelum ada peringkat
- PHD Thesis Ram Dheeraj Business Admin PDFDokumen292 halamanPHD Thesis Ram Dheeraj Business Admin PDFplaycharles89Belum ada peringkat
- Sample: Hospital Authority Do Not Attempt CPR (DNACPR) For Hospitalized PatientsDokumen2 halamanSample: Hospital Authority Do Not Attempt CPR (DNACPR) For Hospitalized PatientsSabilatul AbidahBelum ada peringkat
- Indices and Measurement of Dental CariesDokumen19 halamanIndices and Measurement of Dental Cariesmaher0% (1)
- Breast Cancer Brachytherapy - More ChoicesDokumen5 halamanBreast Cancer Brachytherapy - More ChoicesDr. Robert KuskeBelum ada peringkat
- Contoh Brosur DiabetesDokumen2 halamanContoh Brosur DiabetesRianda FajriFahmiBelum ada peringkat
- SCC Nursing ManagementDokumen2 halamanSCC Nursing ManagementDae HyunBelum ada peringkat