Anda mungkin juga menyukai
- 12.intraoperative Fluid ManagmentDokumen54 halaman12.intraoperative Fluid ManagmentyeabsraBelum ada peringkat
- Colloids and CrystalooidsDokumen42 halamanColloids and Crystalooidsلؤي زعيترBelum ada peringkat
- Review On Peripheral IV FluidsDokumen37 halamanReview On Peripheral IV FluidsWoot RootBelum ada peringkat
- Fluid and Electrolyte ImbalanceDokumen27 halamanFluid and Electrolyte ImbalanceSimmi Sidhu100% (1)
- Nursing Care of Patients Receiving Chemotherapy Ranjita Rajesh Lecturer People's College of Nursing BhopalDokumen55 halamanNursing Care of Patients Receiving Chemotherapy Ranjita Rajesh Lecturer People's College of Nursing BhopalFayizatul AkmarBelum ada peringkat
- NocturiaDokumen10 halamanNocturiaKousik AmancharlaBelum ada peringkat
- Principles of Fluid Therapy On The Basis ofDokumen29 halamanPrinciples of Fluid Therapy On The Basis ofhendrytzBelum ada peringkat
- Fluid & ElectrolyteDokumen69 halamanFluid & ElectrolytePaul Ebenezer100% (1)
- Intradialytic Stretching Exercises On Fatigueand Muscle CrampsDokumen6 halamanIntradialytic Stretching Exercises On Fatigueand Muscle CrampsInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Function of G I System: The Primary Digestive Functions Are Break Down Food Particles "Dokumen113 halamanFunction of G I System: The Primary Digestive Functions Are Break Down Food Particles "cherryann_12100% (1)
- Central Venous PressureDokumen10 halamanCentral Venous PressureAngelo ArquizaBelum ada peringkat
- Management of CholeraDokumen69 halamanManagement of CholeraNatalia LawrenceBelum ada peringkat
- Urine Formation: Reabsorption and Secretion, and Water ConservationDokumen5 halamanUrine Formation: Reabsorption and Secretion, and Water ConservationAshraf Moby100% (1)
- Worksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Dokumen3 halamanWorksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Emerald SpanglerBelum ada peringkat
- Insulin AdministrationDokumen15 halamanInsulin Administrationmec17Belum ada peringkat
- Fluid and ElyctrolyteDokumen49 halamanFluid and Elyctrolyteuuuhbnb lplhghBelum ada peringkat
- Health Assessment in Nursing (LEC) : Prepared By: Mark Joseph V. Liwanag, RN, MSNDokumen43 halamanHealth Assessment in Nursing (LEC) : Prepared By: Mark Joseph V. Liwanag, RN, MSNCj MayoyoBelum ada peringkat
- NKTI Guide to Preventing PD Exit Site InfectionsDokumen35 halamanNKTI Guide to Preventing PD Exit Site InfectionsMarc Pipoy100% (1)
- Chronic Renal Failure TutorialDokumen85 halamanChronic Renal Failure TutorialFrances Rose Cabrera SalongaBelum ada peringkat
- HemiplegiaDokumen17 halamanHemiplegiaStefany CelineBelum ada peringkat
- Intravenous Fluid Therapy in Adults in The HospitalDokumen28 halamanIntravenous Fluid Therapy in Adults in The Hospitalushapadminivadivelswamy100% (2)
- Fluid Management - Presentation PDFDokumen16 halamanFluid Management - Presentation PDFjuniorebinda100% (1)
- FLUIDS AND ELECTROLYTES MNGTDokumen44 halamanFLUIDS AND ELECTROLYTES MNGTremerose100% (1)
- Renal DisordersDokumen77 halamanRenal Disorderslorelee_espaldon100% (1)
- 2018 Overview Digestive System HandoutDokumen11 halaman2018 Overview Digestive System HandoutdraganBelum ada peringkat
- Peritoneal DialysisDokumen23 halamanPeritoneal Dialysismakyofrancis20Belum ada peringkat
- Group 5 - Hemodialysis - Chronic Kidney FailureDokumen31 halamanGroup 5 - Hemodialysis - Chronic Kidney FailureKimberly Abella CabreraBelum ada peringkat
- Optimized Clinical Case StudiesDokumen4 halamanOptimized Clinical Case StudiesAassh DcmbrBelum ada peringkat
- CCJM Symptom Management An Important Part of Cancer CareDokumen10 halamanCCJM Symptom Management An Important Part of Cancer CareBrian HarrisBelum ada peringkat
- Week 11 - Ch. 36 - UrinaryDokumen27 halamanWeek 11 - Ch. 36 - UrinaryMary SingletonBelum ada peringkat
- Disseminated Intravascular CoagulationDokumen17 halamanDisseminated Intravascular Coagulationr DBelum ada peringkat
- Management of Arterial LineDokumen16 halamanManagement of Arterial LineFarcasanu Liana GeorgianaBelum ada peringkat
- Management of Poisoning - Booklet PDFDokumen344 halamanManagement of Poisoning - Booklet PDFkrysteenBelum ada peringkat
- Sepsis Power Point Slide Presentation - The Guidelines - Implementation For The FutureDokumen25 halamanSepsis Power Point Slide Presentation - The Guidelines - Implementation For The Futuremontie13Belum ada peringkat
- Sudden inability to pass urine due to acute urinary retentionDokumen3 halamanSudden inability to pass urine due to acute urinary retentionAgli AdhityaBelum ada peringkat
- Fluid and Electrolyte BalanceDokumen295 halamanFluid and Electrolyte BalanceAnuchithra RadhakrishnanBelum ada peringkat
- Report2014 PDFDokumen332 halamanReport2014 PDFShareDialysis100% (1)
- Insulin Secretion and FunctionDokumen8 halamanInsulin Secretion and FunctionWendy EscalanteBelum ada peringkat
- ENDO... ElectrolyteDokumen44 halamanENDO... ElectrolyteOmar AbdillahiBelum ada peringkat
- IV Infusion SolutionDokumen8 halamanIV Infusion SolutionmohammedBelum ada peringkat
- Lecture Notes On AphDokumen41 halamanLecture Notes On AphEyob MizanBelum ada peringkat
- Fluid and Electrolyte Balance GuideDokumen12 halamanFluid and Electrolyte Balance Guideadadan100% (1)
- Cirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDokumen21 halamanCirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDan ChicinasBelum ada peringkat
- Final Exam PDFDokumen17 halamanFinal Exam PDFirisjames100% (1)
- IV Fluid ChartDokumen2 halamanIV Fluid Charthady920Belum ada peringkat
- Fluid Electrolytes and Acid Base BalanceDokumen108 halamanFluid Electrolytes and Acid Base BalancesayednourBelum ada peringkat
- Physio Reviewer Renal To Acid BaseDokumen11 halamanPhysio Reviewer Renal To Acid BaseNicole ChanBelum ada peringkat
- Fluid Balance in Clinical PracticeDokumen8 halamanFluid Balance in Clinical Practicefernando_vaz2010100% (1)
- Safety of High Alert MedicationDokumen48 halamanSafety of High Alert Medicationrini setyawatiBelum ada peringkat
- Renal Failure PresentationDokumen65 halamanRenal Failure PresentationBhawna JoshiBelum ada peringkat
- Arterial Line Arterial LineDokumen13 halamanArterial Line Arterial LineLinamaria Lozano100% (1)
- Diabetes NotesDokumen10 halamanDiabetes Notestripj33Belum ada peringkat
- IV CalculationsDokumen31 halamanIV CalculationschanaBelum ada peringkat
- Fluids and ElectrolytesDokumen192 halamanFluids and ElectrolytesTeodora JoghiuBelum ada peringkat
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDari EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsBelum ada peringkat
- Icu FluidsDokumen103 halamanIcu FluidsVineel BezawadaBelum ada peringkat
- Maxwell Quick Medical Reference PDFDokumen35 halamanMaxwell Quick Medical Reference PDFAnonymous fj68Ms100% (10)
- Osteolytic LesionsDokumen20 halamanOsteolytic LesionsVineel BezawadaBelum ada peringkat
- Transverse Acetabular Ligament - A Guide To Acetabular Component Anteversion in Total Hip ArthroplastyDokumen5 halamanTransverse Acetabular Ligament - A Guide To Acetabular Component Anteversion in Total Hip ArthroplastyVineel BezawadaBelum ada peringkat
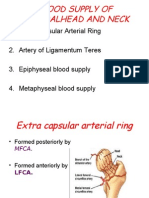
- Blood Supply of Femoral Head and NeckDokumen15 halamanBlood Supply of Femoral Head and NeckVineel BezawadaBelum ada peringkat
- Peo 20051026 IssueDokumen92 halamanPeo 20051026 IssueAlan EscobedoBelum ada peringkat
- Gemmotherapy remedies for detoxification and drainageDokumen2 halamanGemmotherapy remedies for detoxification and drainagesaravan228100% (1)
- Tricorder X PrizeDokumen4 halamanTricorder X PrizemariaBelum ada peringkat
- Fraktur DentoalveolarDokumen25 halamanFraktur DentoalveolarfirmansyahddsBelum ada peringkat
- Process of Elimination: Safety PrincipleDokumen52 halamanProcess of Elimination: Safety Principlejennywatsurproblem100% (1)
- Hricak 2021Dokumen37 halamanHricak 2021Xiomara CelyBelum ada peringkat
- FDA narrative requirements for adverse event reportsDokumen12 halamanFDA narrative requirements for adverse event reportskandulasatish100% (3)
- Caesarean Section Performing Caesarean SectionDokumen13 halamanCaesarean Section Performing Caesarean SectionBlablabla BlablablaBelum ada peringkat
- NCP For Acute Gastroenteritis (Pediatric)Dokumen6 halamanNCP For Acute Gastroenteritis (Pediatric)abcel76% (21)
- CH13 Ninenth Standard NCERT BOOKDokumen26 halamanCH13 Ninenth Standard NCERT BOOKPrash ShanthBelum ada peringkat
- Top 100 Study Items For The Otolaryngology (ENT) Board ExaminationDokumen8 halamanTop 100 Study Items For The Otolaryngology (ENT) Board ExaminationsduxBelum ada peringkat
- Medical CertificateDokumen126 halamanMedical CertificateAnonymous mummYD0% (1)
- Polypharmacy, Interactions and Collaborative Care in The Middle-Aged and Beyond. LB Stargrove and MB Stargrove (2012)Dokumen8 halamanPolypharmacy, Interactions and Collaborative Care in The Middle-Aged and Beyond. LB Stargrove and MB Stargrove (2012)adsfadfsfadafdBelum ada peringkat
- 1.19 Exam PracticeDokumen5 halaman1.19 Exam Practicesunnr008.211Belum ada peringkat
- Section16 - Questions and AnswersDokumen62 halamanSection16 - Questions and Answersdivine venturoBelum ada peringkat
- Prescription AnalysisDokumen16 halamanPrescription AnalysisMohd Azfar HafizBelum ada peringkat
- Obesity Flow ChartDokumen1 halamanObesity Flow Chartmathurarun2000Belum ada peringkat
- Heart Rate LabDokumen6 halamanHeart Rate LabSteve RodriguesBelum ada peringkat
- Efektifitas Latihan Progressive Muscle Relaxation (PMR) Terhadap Mual Muntah Kemoterapi Pasien Kanker OvariumDokumen8 halamanEfektifitas Latihan Progressive Muscle Relaxation (PMR) Terhadap Mual Muntah Kemoterapi Pasien Kanker OvariumMutmin AnsariBelum ada peringkat
- Usp 38 Alt AkkDokumen3 halamanUsp 38 Alt Akkkhoirunnissa hidayatiBelum ada peringkat
- The Federation of Motor Sports Clubs of India 2022 Appendix "B" - Medical HistoryDokumen2 halamanThe Federation of Motor Sports Clubs of India 2022 Appendix "B" - Medical HistoryMBG No.14Belum ada peringkat
- Acquired Brain Injury Early Rehabilitation and Long Term OutcomeDokumen46 halamanAcquired Brain Injury Early Rehabilitation and Long Term OutcomeVeena RaigangarBelum ada peringkat
- Pharmacology of LSD Review (Book Review)Dokumen3 halamanPharmacology of LSD Review (Book Review)Matt BaggottBelum ada peringkat
- Counseling Your Patients About Tobacco Cessation PDFDokumen4 halamanCounseling Your Patients About Tobacco Cessation PDFHamza KhanBelum ada peringkat
- Dermatitis HerpetiformisDokumen4 halamanDermatitis HerpetiformisRizky ArfinaBelum ada peringkat
- Clean Versus Sterile Management of Chronic WoundsDokumen3 halamanClean Versus Sterile Management of Chronic WoundsDon RicaforteBelum ada peringkat
- Multiple-Choice Questions: I Toward Self-Assessment CME. Category 1 CME Credits Not DesigDokumen9 halamanMultiple-Choice Questions: I Toward Self-Assessment CME. Category 1 CME Credits Not DesigManish MauryaBelum ada peringkat
- Blood Culture Manual MT - SinaiDokumen41 halamanBlood Culture Manual MT - SinaiAvi Verma100% (1)
- 142 DefinitionsssDokumen7 halaman142 DefinitionsssAnonymous vXPYrefjGLBelum ada peringkat
- I. The Problem and Its Background Ii. Demand and Analysis Review of Related Literature and Case StudiesDokumen3 halamanI. The Problem and Its Background Ii. Demand and Analysis Review of Related Literature and Case StudiesPaulyn Mae Dela CruzBelum ada peringkat