Anda mungkin juga menyukai
- The Flap Technique For Pocket TherapyDokumen40 halamanThe Flap Technique For Pocket TherapyPrathik RaiBelum ada peringkat
- The Flap Technique For Pocket TherapyDokumen40 halamanThe Flap Technique For Pocket TherapyPrathik RaiBelum ada peringkat
- Periodontal FlapDokumen19 halamanPeriodontal FlapsevattapillaiBelum ada peringkat
- Dr. Zaid Surgical Phase-2Dokumen39 halamanDr. Zaid Surgical Phase-2Abdelrahman GalalBelum ada peringkat
- Periodontal Flap DesignsDokumen68 halamanPeriodontal Flap Designsshazil.21Belum ada peringkat
- The Periodontal Flap: Chap# 57Dokumen45 halamanThe Periodontal Flap: Chap# 57Leena HashmiBelum ada peringkat
- Complications of Exodontics: Mary Cris P EstandarteDokumen49 halamanComplications of Exodontics: Mary Cris P EstandarteRealyn D. BerderaBelum ada peringkat
- Gingival Surgical TechniquesDokumen88 halamanGingival Surgical TechniquesDr. Debbie SabladaBelum ada peringkat
- Principles Of, IncisionsDokumen58 halamanPrinciples Of, Incisionsوليد خالدBelum ada peringkat
- Periodontal FlapsDokumen65 halamanPeriodontal FlapsSaleh AlsadiBelum ada peringkat
- The Periodontal FlapDokumen43 halamanThe Periodontal FlapDeb SBelum ada peringkat
- Periodontal Flaps: DR Sadia Tabassum Asst Prof Optv Dent JMDCDokumen74 halamanPeriodontal Flaps: DR Sadia Tabassum Asst Prof Optv Dent JMDCayesha100% (1)
- Periodontal FlapDokumen64 halamanPeriodontal FlapBlack EyeBelum ada peringkat
- Colgajo Widman ModificadoDokumen7 halamanColgajo Widman ModificadoJohnny CHBelum ada peringkat
- L1 Periodontal Flaps (2) Last L9Dokumen50 halamanL1 Periodontal Flaps (2) Last L9Haneen Al-HajjBelum ada peringkat
- Department of Oral and Maxillofacial Surgery: Goverment Dental College & Hospital, AhmedabadDokumen14 halamanDepartment of Oral and Maxillofacial Surgery: Goverment Dental College & Hospital, AhmedabadkishanBelum ada peringkat
- Preprosthetic SurgeryDokumen22 halamanPreprosthetic Surgeryjerin thomasBelum ada peringkat
- Preprosthetic Surgery MADE EASYDokumen14 halamanPreprosthetic Surgery MADE EASYMohammedBelum ada peringkat
- Flap Surgery and GingivectomyDokumen127 halamanFlap Surgery and GingivectomyPuneet Sachdeva100% (5)
- Rhinoplasty WorkbookDokumen21 halamanRhinoplasty Workbookzena talibBelum ada peringkat
- Periodontal SurgeryDokumen4 halamanPeriodontal SurgeryRinisha SinhaBelum ada peringkat
- Surgical Periodontal TherapyDokumen32 halamanSurgical Periodontal TherapyHaarisBelum ada peringkat
- Perio 5Dokumen7 halamanPerio 5Meiz JaleelBelum ada peringkat
- Surgery of The EyeDokumen3 halamanSurgery of The Eyehonovezaann.a.campita.ctucvmBelum ada peringkat
- Free GINGIVALgraft - The Classic TechniqueDokumen9 halamanFree GINGIVALgraft - The Classic TechniqueMohie Eddine BoudiaBelum ada peringkat
- Principles of Flaps, Suturing and Management of Difficult ExtractionDokumen14 halamanPrinciples of Flaps, Suturing and Management of Difficult ExtractionSRO oOBelum ada peringkat
- CurettageDokumen4 halamanCurettageritika singhBelum ada peringkat
- Surgical Treatment of Diseases of The Maxillary SinusDokumen6 halamanSurgical Treatment of Diseases of The Maxillary SinusRaymund Niño BumatayBelum ada peringkat
- Rhinoplasty 이홍경Dokumen53 halamanRhinoplasty 이홍경entgo8282Belum ada peringkat
- Periodontal Flap Surgery Auto Saved)Dokumen93 halamanPeriodontal Flap Surgery Auto Saved)Raghavendra NaikBelum ada peringkat
- The Periodontal Flap 2Dokumen70 halamanThe Periodontal Flap 2Safaa Ali100% (1)
- Sics Steps: Divisi Katarak Dan Bedah Refraktif Rumah Sakit Mata Bali MandaraDokumen74 halamanSics Steps: Divisi Katarak Dan Bedah Refraktif Rumah Sakit Mata Bali MandaraPande GustianaBelum ada peringkat
- Corrective Phase of Periodontal Therapy (Surgical Phase)Dokumen12 halamanCorrective Phase of Periodontal Therapy (Surgical Phase)Hassan MohamedBelum ada peringkat
- Anophthalmic Socket: OculoplastyDokumen5 halamanAnophthalmic Socket: OculoplastySariShafadenaSiregarBelum ada peringkat
- Presentation By: Dr Saima ( 赛马) N Nakapolo BDS, 4 YearDokumen43 halamanPresentation By: Dr Saima ( 赛马) N Nakapolo BDS, 4 YearIsak ShatikaBelum ada peringkat
- Definition:: Types of Forceps Used For Tooth ExtractionDokumen28 halamanDefinition:: Types of Forceps Used For Tooth Extractionayman moaed alyasen100% (1)
- Minimally Invasive Implant and Sinus Lift Surgery With Immediate LoadingDokumen4 halamanMinimally Invasive Implant and Sinus Lift Surgery With Immediate LoadingrachmadyBelum ada peringkat
- Treatment of Gingiva Recession With A Modified - Tunnel - Technique PDFDokumen7 halamanTreatment of Gingiva Recession With A Modified - Tunnel - Technique PDFFelicia Tsai100% (1)
- Gingivectomy & CurettageDokumen55 halamanGingivectomy & CurettageRajani GedelaBelum ada peringkat
- Basic Implant SurgeryDokumen72 halamanBasic Implant SurgeryKandiwapa100% (2)
- Procedure: Elevation of FlapDokumen2 halamanProcedure: Elevation of FlapGhinalya Chalbi AnandaBelum ada peringkat
- Incision, Flap, SuturingDokumen79 halamanIncision, Flap, Suturingyashobantab2021Belum ada peringkat
- Free FlapDokumen19 halamanFree FlaperinastevianaBelum ada peringkat
- Dental Implants PerioDokumen81 halamanDental Implants PerioSaba KhanBelum ada peringkat
- Preprosthetic Surgery 4th Year LectureDokumen57 halamanPreprosthetic Surgery 4th Year Lectureمحمد يوسف المصراتيBelum ada peringkat
- تسنيم شمالي -frenectomyDokumen35 halamanتسنيم شمالي -frenectomyTasneem ShamaliBelum ada peringkat
- Reyneke2015.PDF Bsso StepsDokumen10 halamanReyneke2015.PDF Bsso StepsBenjie LawBelum ada peringkat
- Gingival CurettageDokumen22 halamanGingival CurettagePrathik RaiBelum ada peringkat
- Temporal Bone Dissection ManualDokumen15 halamanTemporal Bone Dissection Manualabhi2537100% (1)
- Pre-Prosthetic SurgeryDokumen61 halamanPre-Prosthetic SurgeryAswitha GanapathyBelum ada peringkat
- Dr. Diana Mostafa Abo El OlaDokumen68 halamanDr. Diana Mostafa Abo El Olasohaib natshehBelum ada peringkat
- Nasal Septal PerforationDokumen13 halamanNasal Septal PerforationDr. T. Balasubramanian75% (4)
- Flap Design For Minor SurgeryDokumen10 halamanFlap Design For Minor SurgeryOchtavianusBelum ada peringkat
- Abhi ProsthoDokumen60 halamanAbhi ProsthoHashifvc AliBelum ada peringkat
- Mucogingival Surgery IDokumen32 halamanMucogingival Surgery IMayleen LeeBelum ada peringkat
- White Intumescent Cataract Management: My Approach: 2022, #1Dari EverandWhite Intumescent Cataract Management: My Approach: 2022, #1Belum ada peringkat
- Cataract And Small Pupil Management Manual Techniques: 2022, #1Dari EverandCataract And Small Pupil Management Manual Techniques: 2022, #1Belum ada peringkat
- Posterior Polar Cataract Management: My Approach: 2022, #1Dari EverandPosterior Polar Cataract Management: My Approach: 2022, #1Belum ada peringkat
- MCQs in Oral Surgery: A comprehensive reviewDari EverandMCQs in Oral Surgery: A comprehensive reviewPenilaian: 5 dari 5 bintang5/5 (6)
- A Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersDari EverandA Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersBelum ada peringkat
- Effectiveness of Micronutrients and Physiotherapy in The Management of Oral Submucous Fibrosis PDFDokumen5 halamanEffectiveness of Micronutrients and Physiotherapy in The Management of Oral Submucous Fibrosis PDFNia LieantoBelum ada peringkat
- Aribex BrochureDokumen3 halamanAribex BrochureNia LieantoBelum ada peringkat
- Article 1459955174Dokumen9 halamanArticle 1459955174Nia LieantoBelum ada peringkat
- Nonsurgical RetreatmentDokumen4 halamanNonsurgical RetreatmentNia LieantoBelum ada peringkat
- 1 SMDokumen6 halaman1 SMNia LieantoBelum ada peringkat
- Introduction To PeriodonticsDokumen28 halamanIntroduction To PeriodonticsHeba S Radaideh100% (3)
- Brazilian Board of Orthodontics and Facial Orthopedics: Certifying ExcellenceDokumen10 halamanBrazilian Board of Orthodontics and Facial Orthopedics: Certifying ExcellenceHanindyaNoorAgusthaBelum ada peringkat
- Tutorial 8 Animal NutritionDokumen21 halamanTutorial 8 Animal Nutritionoasis_dessertBelum ada peringkat
- Roth Versus MBTDokumen8 halamanRoth Versus MBTAurora MartinezBelum ada peringkat
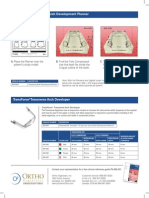
- TransForce®2 Transverse Arch Development PlannerDokumen2 halamanTransForce®2 Transverse Arch Development PlannerOrtho OrganizersBelum ada peringkat
- 2nd Anoucment Sini 3 PDFDokumen2 halaman2nd Anoucment Sini 3 PDFBudiono WijayaBelum ada peringkat
- Fungsi Lain Waterlase PDFDokumen42 halamanFungsi Lain Waterlase PDFJunk Bayu KacingBelum ada peringkat
- 1 s2.0 S2212443823000371 MainDokumen11 halaman1 s2.0 S2212443823000371 MainMirza GlusacBelum ada peringkat
- مصطلحات طب الاسنان dental termsDokumen15 halamanمصطلحات طب الاسنان dental termsAyedAlfalah100% (1)
- The Operating Field Presenter Mustapha Danjuma Abubakar 6 Year DMD 0ctober 2021Dokumen23 halamanThe Operating Field Presenter Mustapha Danjuma Abubakar 6 Year DMD 0ctober 2021jamaica faith ramonBelum ada peringkat
- Bad Habits That Cause Your Dental Implants To FailDokumen2 halamanBad Habits That Cause Your Dental Implants To FailDentist at False CreekBelum ada peringkat
- Wire BendingDokumen165 halamanWire BendingArsalah Raffat96% (28)
- Immediate Implant Placement FollowingDokumen3 halamanImmediate Implant Placement FollowingHarsh ChansoriaBelum ada peringkat
- Tunnel Access For Guided Bone Regeneration in The Maxillary AnteriorDokumen6 halamanTunnel Access For Guided Bone Regeneration in The Maxillary Anteriormax100% (1)
- No No Registrasi Tanggal Registrasi Jenis Pelayanan Nama DokterDokumen13 halamanNo No Registrasi Tanggal Registrasi Jenis Pelayanan Nama Doktertegar permadiBelum ada peringkat
- Bragger 1992 - Surgical CLDokumen7 halamanBragger 1992 - Surgical CLBryan HeeBelum ada peringkat
- قائمة الكتبDokumen18 halamanقائمة الكتبخالدعلمBelum ada peringkat
- Carriere Distalizer Invisalign ArticleDokumen4 halamanCarriere Distalizer Invisalign ArticleOrtho Organizers100% (1)
- Functional Occlusion: Presented By-Dr. Ruchi Saxena Dept. of OrthodonticsDokumen186 halamanFunctional Occlusion: Presented By-Dr. Ruchi Saxena Dept. of OrthodonticsDrkishore Reddy0% (1)
- Sato - Manual Basic MeawDokumen156 halamanSato - Manual Basic MeawNhock LamentosBelum ada peringkat
- Complete Denture Prosthodontics Manappallil PDF FreeDokumen3 halamanComplete Denture Prosthodontics Manappallil PDF FreeJannatulBelum ada peringkat
- Oral Habits in School Going Children of Delhi: A Prevalence StudyDokumen5 halamanOral Habits in School Going Children of Delhi: A Prevalence StudyStacia AnastashaBelum ada peringkat
- Clinical Case Reports - 2023 - Vyver - Apexification of Dens Evaginatus in A Mandibular Premolar A Case ReportDokumen6 halamanClinical Case Reports - 2023 - Vyver - Apexification of Dens Evaginatus in A Mandibular Premolar A Case ReportIqra KhanBelum ada peringkat
- Dental Anthropology: September 2017Dokumen9 halamanDental Anthropology: September 2017Amira IzzatusyuhadaBelum ada peringkat
- Linear OcclusionDokumen8 halamanLinear OcclusionAmar BhochhibhoyaBelum ada peringkat
- Soft Tissue Clinical and Cephalometric AnalysisDokumen145 halamanSoft Tissue Clinical and Cephalometric Analysisvelangni50% (2)
- PULPITISDokumen35 halamanPULPITISapi-19916399Belum ada peringkat
- First Order Second OrderDokumen12 halamanFirst Order Second OrderSrishti Syal50% (2)
- Paramjit Kaur - Oral Cavity of NeonatesDokumen27 halamanParamjit Kaur - Oral Cavity of Neonatesdr parveen bathlaBelum ada peringkat
- Alinhamento Inferior Arcos JulioDokumen6 halamanAlinhamento Inferior Arcos JulioDiego Andres Hincapie HerreraBelum ada peringkat