Anda mungkin juga menyukai
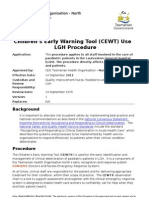
- Children's Early Warning ToolDokumen7 halamanChildren's Early Warning ToolYwagar YwagarBelum ada peringkat
- Patient Progress Note ProtocolDokumen8 halamanPatient Progress Note ProtocolVito Wilfredo100% (1)
- Integrated Hospital Management SystemDokumen5 halamanIntegrated Hospital Management Systemabhi_sbitBelum ada peringkat
- PrescriptionDokumen2 halamanPrescriptionELvin LozandeBelum ada peringkat
- Resume - RaheelaDokumen1 halamanResume - Raheelaapi-490760895Belum ada peringkat
- Medical Records: Standard MOI.9Dokumen5 halamanMedical Records: Standard MOI.9Azza FaroukBelum ada peringkat
- Autistic Disturbances of Affective Contact Kanner 1943Dokumen36 halamanAutistic Disturbances of Affective Contact Kanner 1943AlexantrBelum ada peringkat
- MediSafe Infinite PDFDokumen21 halamanMediSafe Infinite PDFNazim SalehBelum ada peringkat
- COP 1 and 2Dokumen16 halamanCOP 1 and 2Kristel Jane QuitoBelum ada peringkat
- Health Records: Organization and Management of Medical Record DepartmentDokumen24 halamanHealth Records: Organization and Management of Medical Record Departmentosama rf100% (1)
- Documentation and ReportingDokumen17 halamanDocumentation and Reportingsonam MaclayBelum ada peringkat
- MRD/ Clinical Information UnitDokumen21 halamanMRD/ Clinical Information UnitMohd SalahuddinBelum ada peringkat
- GUIDELINES AND PROTOCOLS IN DOCUMENTATION - HceDokumen5 halamanGUIDELINES AND PROTOCOLS IN DOCUMENTATION - HceRoshin TejeroBelum ada peringkat
- Hospital ManagementDokumen20 halamanHospital ManagementGokulBelum ada peringkat
- 13 ElectronicHealthRecordDokumen48 halaman13 ElectronicHealthRecordkimchi girl100% (1)
- Information Desk ModuleDokumen7 halamanInformation Desk Moduleyokes waranBelum ada peringkat
- Medical Records Doc GuideDokumen51 halamanMedical Records Doc Guidealwy aliBelum ada peringkat
- Chapter 3 - Medical Record ProceduresDokumen17 halamanChapter 3 - Medical Record ProceduresLalita A/P AnbarasenBelum ada peringkat
- Project Name: Online Healthcare System Project Course: Object Oriented Analysis and Design Course Teacher: MD. ANWARUL KABIRDokumen7 halamanProject Name: Online Healthcare System Project Course: Object Oriented Analysis and Design Course Teacher: MD. ANWARUL KABIRSadmanMahfuzBelum ada peringkat
- Bab 3 - 07-106Dokumen21 halamanBab 3 - 07-106kolokoyisnearbyBelum ada peringkat
- EHR_3fc5f2f54f015fb95234d66cec45b30eDokumen64 halamanEHR_3fc5f2f54f015fb95234d66cec45b30esaurabh chaturvediBelum ada peringkat
- MODULE 3 STUDENT National Patient Safety Goals 2013Dokumen15 halamanMODULE 3 STUDENT National Patient Safety Goals 2013Dewi Ratna Sari100% (1)
- Hospital Management Information SystemDokumen22 halamanHospital Management Information SystemLakshmi Rj100% (1)
- Pharmacy Management SystemDokumen4 halamanPharmacy Management SystemTaniya FernandoBelum ada peringkat
- Clinical information systems 2 (1)Dokumen33 halamanClinical information systems 2 (1)Rashmi SainiBelum ada peringkat
- HMS SRS for xyz HospitalDokumen6 halamanHMS SRS for xyz HospitalSania JavaidBelum ada peringkat
- Hospital ManagementDokumen29 halamanHospital ManagementRohit YadavBelum ada peringkat
- Physician Care ManagerDokumen3 halamanPhysician Care Managerkman0722Belum ada peringkat
- Hospital ManagementDokumen34 halamanHospital ManagementNavin JethwaniBelum ada peringkat
- Critical Care Applications: Karen Donaire Mary GeraliDokumen20 halamanCritical Care Applications: Karen Donaire Mary GeraliKaren Mae Ü DonaireBelum ada peringkat
- Hospital Information System: AdvantagesDokumen19 halamanHospital Information System: AdvantagesDenisa CekreziBelum ada peringkat
- Reporting in Nursing: By: ImavikeDokumen16 halamanReporting in Nursing: By: ImavikererenrahmawatiBelum ada peringkat
- Nusing InformaticsmbondaDokumen16 halamanNusing Informaticsmbondaapi-302722623Belum ada peringkat
- Hospital Management System For Mayo Clinic: Prepared By: KISHOR KUNALDokumen12 halamanHospital Management System For Mayo Clinic: Prepared By: KISHOR KUNALRohit Krishnan MBelum ada peringkat
- 5-HMIS Components Basic Functions v1Dokumen36 halaman5-HMIS Components Basic Functions v1TheOnePT84% (19)
- Medical RecordsDokumen19 halamanMedical RecordsgurupathiBelum ada peringkat
- 13 ClinicalsummariesDokumen2 halaman13 Clinicalsummariesapi-101814919Belum ada peringkat
- Application of computer in pharmacyDokumen4 halamanApplication of computer in pharmacybryankachocho17Belum ada peringkat
- Pharmacy Service Improvement at CVSDokumen2 halamanPharmacy Service Improvement at CVSHimanshu KumarBelum ada peringkat
- Role of Computer in HospitalsDokumen50 halamanRole of Computer in HospitalsLaiba KhalidBelum ada peringkat
- Joint Commission Medical Record Documentation Requirements 2011Dokumen1 halamanJoint Commission Medical Record Documentation Requirements 2011ronaldrey_007Belum ada peringkat
- Unit Dose SystemDokumen38 halamanUnit Dose SystemluisynonBelum ada peringkat
- Medical Record Department: Ravi Bagali Jayendra Tripati Amrithayan Das Shivaram Gaurav RaviDokumen61 halamanMedical Record Department: Ravi Bagali Jayendra Tripati Amrithayan Das Shivaram Gaurav RaviRashid AyubiBelum ada peringkat
- Chapter 8Dokumen30 halamanChapter 8ankitmanash0% (1)
- AccreditationReadiness Booklet (Version 1.0) - May 2022Dokumen44 halamanAccreditationReadiness Booklet (Version 1.0) - May 2022Leon GuerreroBelum ada peringkat
- Hospital Information System Hand OutDokumen6 halamanHospital Information System Hand OutArlyn CastroBelum ada peringkat
- Hospital 9Dokumen15 halamanHospital 9shaista siddiqueBelum ada peringkat
- Him Paper: Jackqulynn PaigeDokumen10 halamanHim Paper: Jackqulynn PaigeAladyiaBelum ada peringkat
- Ortho PresentationDokumen10 halamanOrtho PresentationarchanaBelum ada peringkat
- Back Up Plan 3Dokumen3 halamanBack Up Plan 3api-315915714Belum ada peringkat
- Synopsis of Hospital Billing SystemDokumen9 halamanSynopsis of Hospital Billing SystemAshutosh JhaBelum ada peringkat
- Software Requirement Specification Hospital Management SystemDokumen55 halamanSoftware Requirement Specification Hospital Management SystemParisakhanBelum ada peringkat
- Lesson 9 HIS Hospital Information SystemDokumen36 halamanLesson 9 HIS Hospital Information SystemKauline Joseph C. BrionesBelum ada peringkat
- Learning Module NUMBER 4 FilingTracking and Retention of Health RecordsDokumen25 halamanLearning Module NUMBER 4 FilingTracking and Retention of Health RecordsHappee AppsBelum ada peringkat
- Med ReportDokumen9 halamanMed ReportAanam FathimaBelum ada peringkat
- Critical Care ApplicationDokumen49 halamanCritical Care ApplicationGracy CasañaBelum ada peringkat
- All Softeng RequirementsDokumen8 halamanAll Softeng RequirementsRAYMART BONAGUABelum ada peringkat
- Presentation (4) - 1Dokumen27 halamanPresentation (4) - 1Kartik Patil100% (1)
- Se Case StudyDokumen14 halamanSe Case Studyharsh.guptacomp22Belum ada peringkat
- Management Information System in The HealthcareDokumen5 halamanManagement Information System in The HealthcaredominicjimenezBelum ada peringkat
- Hospital Management System ProposalDokumen11 halamanHospital Management System ProposalYaminKhanBelum ada peringkat
- Online Hospital ManagementDokumen9 halamanOnline Hospital ManagementWahidul IslamBelum ada peringkat
- SRS For CMS ENDokumen4 halamanSRS For CMS ENMohammed AlshamiBelum ada peringkat
- 1.1) Purpose: Hospital Management SystemDokumen4 halaman1.1) Purpose: Hospital Management SystemdynaestrebillaBelum ada peringkat
- Textbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipDari EverandTextbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Datacom Report for SOMELEC in NOAKCHOTTDokumen1 halamanDatacom Report for SOMELEC in NOAKCHOTTmeddouBelum ada peringkat
- E1/T1 Test Report: Port A: Global ResultsDokumen1 halamanE1/T1 Test Report: Port A: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- E1/T1 Test Report: Port A: Global ResultsDokumen1 halamanE1/T1 Test Report: Port A: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- ZXMW pr10 S400amps500Dokumen44 halamanZXMW pr10 S400amps500meddouBelum ada peringkat
- Software Documentation: Written By: Ian Sommerville Presentation By: Stephen Lopez-CoutoDokumen24 halamanSoftware Documentation: Written By: Ian Sommerville Presentation By: Stephen Lopez-CoutoAshish BholeBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Adderlink X50 & X50-Ms: Video and Usb Over 50MDokumen2 halamanAdderlink X50 & X50-Ms: Video and Usb Over 50MmeddouBelum ada peringkat
- E1/T1 Test Report: Port A: Global ResultsDokumen1 halamanE1/T1 Test Report: Port A: Global ResultsmeddouBelum ada peringkat
- Datacom Report: Global ResultsDokumen1 halamanDatacom Report: Global ResultsmeddouBelum ada peringkat
- Diabetic Patient Suffers Tissue Damage During Interfacility TransportDokumen38 halamanDiabetic Patient Suffers Tissue Damage During Interfacility TransportmeddouBelum ada peringkat
- PraveenDokumen19 halamanPraveenaghorbanzadehBelum ada peringkat
- E1/T1 Test Report: Port A: Global ResultsDokumen1 halamanE1/T1 Test Report: Port A: Global ResultsmeddouBelum ada peringkat
- Adder: AL Extender PairDokumen54 halamanAdder: AL Extender PairmeddouBelum ada peringkat
- Requirements Documentation 2005Dokumen47 halamanRequirements Documentation 2005meddouBelum ada peringkat
- An Interactive Approach To Good Clinical Practices (GCPS) : Brandi N. Ring, M.A. Boston University School of MedicineDokumen57 halamanAn Interactive Approach To Good Clinical Practices (GCPS) : Brandi N. Ring, M.A. Boston University School of MedicinemeddouBelum ada peringkat
- Process DocumentationDokumen36 halamanProcess DocumentationSayd FadelBelum ada peringkat
- Process and Procedure Documentation OverviewDokumen14 halamanProcess and Procedure Documentation OverviewmeddouBelum ada peringkat
- Ayurvedic Health & Wellness Center - Divyarishi Arogyam SansthanDokumen3 halamanAyurvedic Health & Wellness Center - Divyarishi Arogyam SansthandivyarishiBelum ada peringkat
- Patient Satisfaction SurveyDokumen113 halamanPatient Satisfaction SurveyCherry Mae L. Villanueva100% (1)
- Vaatsalya Hospitals: Presented by - Ashish Kumar Singh Anantvijay Sharma Jasmeet Narvekar Mriganka Parashar Nitasha SainiDokumen19 halamanVaatsalya Hospitals: Presented by - Ashish Kumar Singh Anantvijay Sharma Jasmeet Narvekar Mriganka Parashar Nitasha SainiAshish SinghBelum ada peringkat
- Comprensión Escrita 1: LauraDokumen3 halamanComprensión Escrita 1: LauraSonia Garcia DiazBelum ada peringkat
- Helping Hospitalized Children Feel Less Afraid: The Role of the MEDi RobotDokumen2 halamanHelping Hospitalized Children Feel Less Afraid: The Role of the MEDi RobotYolanda CspBelum ada peringkat
- Orogastric Tube InsertionDokumen5 halamanOrogastric Tube InsertionUday KumarBelum ada peringkat
- PSG Medical RecordsDokumen8 halamanPSG Medical RecordsdavisBelum ada peringkat
- PNF BrochureDokumen5 halamanPNF BrochuredariandBelum ada peringkat
- Nursing History Timeline Key EventsDokumen13 halamanNursing History Timeline Key EventsRosemarie EustaquioBelum ada peringkat
- NDS Study Club Brochure v4Dokumen9 halamanNDS Study Club Brochure v4Hamed KarimiBelum ada peringkat
- Bahan Pagets Disease of MaxillaDokumen3 halamanBahan Pagets Disease of MaxillayuniBelum ada peringkat
- Eosinophilic Granulomatosis With Polyangiitis Associated With Subcutaneous Nodules in A 10-Year-Old GirDokumen2 halamanEosinophilic Granulomatosis With Polyangiitis Associated With Subcutaneous Nodules in A 10-Year-Old GirShelyAzradBelum ada peringkat
- Sneha Nirav Marjadi V State of Maharashtra Ors and Connected PetitionsDokumen16 halamanSneha Nirav Marjadi V State of Maharashtra Ors and Connected PetitionsNek PuriBelum ada peringkat
- Humanitarian Assisstance of Mormon Church in SerbiaDokumen8 halamanHumanitarian Assisstance of Mormon Church in SerbiaSasa MilosevicBelum ada peringkat
- Stoma CounselingDokumen5 halamanStoma CounselingFitriana HermanBelum ada peringkat
- Best Docs - Aug 09Dokumen18 halamanBest Docs - Aug 09AY Magazine100% (2)
- Revalidation Forms CombinedDokumen12 halamanRevalidation Forms CombinedG RobinsonBelum ada peringkat
- Jaundice Meter JM-105 Gentle For The Newborn, Efficient For YouDokumen8 halamanJaundice Meter JM-105 Gentle For The Newborn, Efficient For YouFernando RumapeaBelum ada peringkat
- India Bradley Curriculum Vitae WeeblyDokumen3 halamanIndia Bradley Curriculum Vitae Weeblyapi-251445536Belum ada peringkat
- Nurse's Practice Concerning Mouth Care For Unconscious or Debilitated PatientDokumen5 halamanNurse's Practice Concerning Mouth Care For Unconscious or Debilitated PatientFikri IramaBelum ada peringkat
- Billno Duedate DatereceivedDokumen24 halamanBillno Duedate DatereceivedEijizer Zion NarcisoBelum ada peringkat
- Titles of CandidatesDokumen13 halamanTitles of CandidatessanolBelum ada peringkat
- Guidelines For Patients On Chronic Haemodialysis Programme QehbDokumen33 halamanGuidelines For Patients On Chronic Haemodialysis Programme QehbRhys Espinosa100% (2)
- Patient Data Sheet: General Appearance: RespiratoryDokumen5 halamanPatient Data Sheet: General Appearance: RespiratoryAshley SutherlandBelum ada peringkat
- Abadar Medical CenterDokumen2 halamanAbadar Medical CenterEgas Pinto BastoBelum ada peringkat