Anda mungkin juga menyukai
- Social and Administrative Aspects of Pharmacy in Low- and Middle-Income Countries: Present Challenges and Future SolutionsDari EverandSocial and Administrative Aspects of Pharmacy in Low- and Middle-Income Countries: Present Challenges and Future SolutionsPenilaian: 1 dari 5 bintang1/5 (1)
- Medicine Price Surveys, Analyses and Comparisons: Evidence and Methodology GuidanceDari EverandMedicine Price Surveys, Analyses and Comparisons: Evidence and Methodology GuidanceSabine VoglerBelum ada peringkat
- Drug Therapy MonitoringDokumen48 halamanDrug Therapy MonitoringPooja agarwalBelum ada peringkat
- 023-Rational Use of DrugsDokumen43 halaman023-Rational Use of DrugsfikebatuBelum ada peringkat
- Pharmacotherapeutics UNIT1Dokumen44 halamanPharmacotherapeutics UNIT1Bharti ChauhanBelum ada peringkat
- Hospital Formulary-Lecture NotesDokumen7 halamanHospital Formulary-Lecture NotesPatras BhattiBelum ada peringkat
- Rational Use of Drugs-IDokumen38 halamanRational Use of Drugs-IUmair Mazhar100% (1)
- New Concept of Pharmacy PracticeDokumen21 halamanNew Concept of Pharmacy PracticeSaddamix AL OmariBelum ada peringkat
- 1 - Pharmaceutical Care Practice - An OverviewDokumen76 halaman1 - Pharmaceutical Care Practice - An OverviewekramBelum ada peringkat
- Community Pharmacy ManagementDokumen10 halamanCommunity Pharmacy ManagementAnkit DhoreBelum ada peringkat
- Immunization Policy Guidline - Kenya 2013Dokumen72 halamanImmunization Policy Guidline - Kenya 2013okwadha simionBelum ada peringkat
- Disp MEDICATION ADHERENCE and DISPENSING PROCESSDokumen28 halamanDisp MEDICATION ADHERENCE and DISPENSING PROCESSPius VillarBelum ada peringkat
- Lecture 1. Introduction To Clinical PharmacyDokumen14 halamanLecture 1. Introduction To Clinical Pharmacydaniya nadeem100% (1)
- Community Pharmacy PracticeDokumen18 halamanCommunity Pharmacy Practiceكسلان اكتب اسميBelum ada peringkat
- Labelling and PackagingDokumen16 halamanLabelling and PackagingvyshnosudhaBelum ada peringkat
- Medication HistoryDokumen19 halamanMedication HistoryAnisha PandeyBelum ada peringkat
- Introduction To Pharmacoepidemiology PDFDokumen17 halamanIntroduction To Pharmacoepidemiology PDFRhiny Erfiah RhindaBelum ada peringkat
- Chapter 2 PEY-Measurement of Outcomes - Pharma DostDokumen50 halamanChapter 2 PEY-Measurement of Outcomes - Pharma DostKhadeer AG50% (2)
- Pharmacy InternsDokumen14 halamanPharmacy InternsJames LindonBelum ada peringkat
- Bronchodilator & Other Drugs Used in AsthmaDokumen15 halamanBronchodilator & Other Drugs Used in AsthmaGenta JagadBelum ada peringkat
- Pharmacists Role Clinical Pharmacokinetic MonitoringDokumen2 halamanPharmacists Role Clinical Pharmacokinetic MonitoringauliaBelum ada peringkat
- Institutional Pharmacy PracticeDokumen17 halamanInstitutional Pharmacy PracticeRichmond AmuraoBelum ada peringkat
- Guide To Good Dispensing PracticeDokumen7 halamanGuide To Good Dispensing PracticeGizelle Mae Pasiol-MacayanBelum ada peringkat
- Community PharmacyDokumen8 halamanCommunity PharmacyAmit KumarBelum ada peringkat
- Introduction To Pharmacoepidemiology 2015 PDFDokumen20 halamanIntroduction To Pharmacoepidemiology 2015 PDFNovria Rizki HarahapBelum ada peringkat
- Drug Categorizatio RULEDokumen27 halamanDrug Categorizatio RULEDIPENDRA CHAUDHARYBelum ada peringkat
- Ward RoundDokumen2 halamanWard RoundAnonymous whcvnPBeQBelum ada peringkat
- Adverse Drug Reactions NotesDokumen4 halamanAdverse Drug Reactions NoteskarthikeyanpgtBelum ada peringkat
- Patient Medication Profile and CounselingDokumen56 halamanPatient Medication Profile and CounselingMeimei QueBelum ada peringkat
- Modified Systematic Approach To Answering QuestionsDokumen5 halamanModified Systematic Approach To Answering QuestionsromeofatimaBelum ada peringkat
- Procurement and WarehouseDokumen28 halamanProcurement and WarehouseVarshith Gandla100% (1)
- Clinical Pharmacy - A Definition: Fahad Hussain 9/20/2010Dokumen4 halamanClinical Pharmacy - A Definition: Fahad Hussain 9/20/2010Tawhida Islam100% (1)
- Activity 1 DDS LABDokumen96 halamanActivity 1 DDS LABChristine RanoaBelum ada peringkat
- 2 Conversion of Iv To PoDokumen27 halaman2 Conversion of Iv To PoSreya Sanil100% (1)
- Pharmacotherapy of HTNDokumen57 halamanPharmacotherapy of HTNAbera JamboBelum ada peringkat
- Procurement and Inventory ManagementDokumen43 halamanProcurement and Inventory ManagementSAURABH SINGHBelum ada peringkat
- Patient Medication History Interview: Dr. Vijay B. Lambole Associate Professor, SNLPCP, UmrakhDokumen20 halamanPatient Medication History Interview: Dr. Vijay B. Lambole Associate Professor, SNLPCP, Umrakhvijaylambole0% (1)
- Dispensing ChecklistDokumen2 halamanDispensing Checklistsafia321Belum ada peringkat
- Chapter 1 - Pharma DostDokumen3 halamanChapter 1 - Pharma DostabinchandrakumarBelum ada peringkat
- Experiential Pharmacy Practice in Institutional Pharmacy: Module 1: Part 2Dokumen27 halamanExperiential Pharmacy Practice in Institutional Pharmacy: Module 1: Part 2levi pinedaBelum ada peringkat
- Hospital Pharmacy Communication NewsletterDokumen6 halamanHospital Pharmacy Communication NewsletterHarsh Bhardwaj0% (1)
- Adverse Drug ReactionDokumen24 halamanAdverse Drug ReactionGopal pokhrelBelum ada peringkat
- Rational Use of AntibioticsDokumen26 halamanRational Use of AntibioticsDr-Jagadeesh MangamooriBelum ada peringkat
- Drug Information Resources PDFDokumen68 halamanDrug Information Resources PDFhark reynaldo100% (1)
- Application of PK in Clinical SitutionDokumen42 halamanApplication of PK in Clinical Situtionsafia mehmood100% (1)
- Exercises 8-10 (By Dr. N. Tubon) PDFDokumen25 halamanExercises 8-10 (By Dr. N. Tubon) PDFLoren100% (1)
- Drug Related ProblemsDokumen40 halamanDrug Related Problemsfauzul husnaBelum ada peringkat
- M2 - Lesson 1 - Preparation of Standard Patient ScriptingDokumen22 halamanM2 - Lesson 1 - Preparation of Standard Patient ScriptingElleason Joshua G. FranciscoBelum ada peringkat
- Ethics in Pharmaceutical IssuesDokumen21 halamanEthics in Pharmaceutical IssuesAnaliza Kitongan LantayanBelum ada peringkat
- Clinical PharmacyDokumen15 halamanClinical PharmacyKate EvangelistaBelum ada peringkat
- Hospital and Clinical PharmacyDokumen15 halamanHospital and Clinical PharmacyPoonam Verma100% (2)
- Ward Round Participation & Drug Therapy MonitoringDokumen20 halamanWard Round Participation & Drug Therapy MonitoringAman UpadhyayBelum ada peringkat
- Hospital PharmacyDokumen2 halamanHospital Pharmacyomarii67% (3)
- 1 Scope of Pharmacology PDFDokumen5 halaman1 Scope of Pharmacology PDFPaulo Rhoven Navarro Ranay100% (1)
- Manual of CP & Internship ClerkshipDokumen9 halamanManual of CP & Internship Clerkshipsri deepika sri deepikaBelum ada peringkat
- Comunity Pharmacy Introduction ModDokumen42 halamanComunity Pharmacy Introduction ModPrity girlBelum ada peringkat
- Introduction To Pharmacy PracticeDokumen9 halamanIntroduction To Pharmacy PracticeRai Waqas100% (1)
- Developing Pharmacy Practice - WHO - PSM - PAR - 2006.5 PDFDokumen97 halamanDeveloping Pharmacy Practice - WHO - PSM - PAR - 2006.5 PDFYuly YusBelum ada peringkat
- Module 4 HOSPITAL PHARMACY WITH INTERPROFESSIONAL APPROACHDokumen18 halamanModule 4 HOSPITAL PHARMACY WITH INTERPROFESSIONAL APPROACHNathalie OmeroBelum ada peringkat
- Chapter 1 - AnswersDokumen5 halamanChapter 1 - AnswersYuvashree KalaiBelum ada peringkat
- CHAPTER 07 Managing Employee Motivation and PerformanceDokumen25 halamanCHAPTER 07 Managing Employee Motivation and PerformanceAnonymous DgPsK0oQBelum ada peringkat
- CHAPTER 10 The Controlling ProcessDokumen26 halamanCHAPTER 10 The Controlling ProcessAnonymous DgPsK0oQBelum ada peringkat
- Basic Elements If Individual BehaviorDokumen29 halamanBasic Elements If Individual BehaviorA. K. MohiuddinBelum ada peringkat
- C7 Managing Leadership and Influence ProcessDokumen26 halamanC7 Managing Leadership and Influence ProcessA. K. MohiuddinBelum ada peringkat
- CHAPTER 01 Managing The Managers JobDokumen35 halamanCHAPTER 01 Managing The Managers JobAnonymous DgPsK0oQ100% (1)
- CHPT 2Dokumen60 halamanCHPT 2Asif NawazBelum ada peringkat
- 6.chap06 Strategy Choice FredDokumen18 halaman6.chap06 Strategy Choice FredAnonymous DgPsK0oQBelum ada peringkat
- CGAPTER 06 MANAGING Organization Change and InnovationDokumen25 halamanCGAPTER 06 MANAGING Organization Change and InnovationAnonymous DgPsK0oQBelum ada peringkat
- CHAPTER 04 Managing Decision Making and ProbDokumen24 halamanCHAPTER 04 Managing Decision Making and ProbAnonymous DgPsK0oQBelum ada peringkat
- 7.chap 7 Implementation Strategy FredDokumen13 halaman7.chap 7 Implementation Strategy FredAnonymous DgPsK0oQBelum ada peringkat
- Cgapter 05 Basic Elements of OrganizingDokumen27 halamanCgapter 05 Basic Elements of OrganizingAnonymous DgPsK0oQBelum ada peringkat
- L5 Product PromotionDokumen11 halamanL5 Product PromotionAnonymous DgPsK0oQBelum ada peringkat
- Chapter 03 Basic Elements of PlanningDokumen23 halamanChapter 03 Basic Elements of PlanningAnonymous DgPsK0oQBelum ada peringkat
- 8.chap 8 Strategy Review FredDokumen16 halaman8.chap 8 Strategy Review FredAnonymous DgPsK0oQBelum ada peringkat
- Musculoskeletal CDokumen29 halamanMusculoskeletal CAnonymous DgPsK0oQBelum ada peringkat
- 5.chap05 Strategy in Action FredDokumen51 halaman5.chap05 Strategy in Action FredAnonymous DgPsK0oQBelum ada peringkat
- 4.chapr04 Internal Analysis RobinsonDokumen11 halaman4.chapr04 Internal Analysis RobinsonAnonymous DgPsK0oQBelum ada peringkat
- Topical Preparations InorganicDokumen12 halamanTopical Preparations InorganicAnonymous DgPsK0oQBelum ada peringkat
- 1 Chap01IntroductionDokumen28 halaman1 Chap01IntroductionAnonymous DgPsK0oQBelum ada peringkat
- The Business Vision & Mission: Strategic Management: Concepts & CasesDokumen17 halamanThe Business Vision & Mission: Strategic Management: Concepts & CasesAnonymous DgPsK0oQBelum ada peringkat
- Complimentary MedicineDokumen3 halamanComplimentary MedicineAnonymous DgPsK0oQBelum ada peringkat
- L6 Brand Building Brand ManagementDokumen5 halamanL6 Brand Building Brand ManagementAnonymous DgPsK0oQBelum ada peringkat
- Dermatology: Figure: Diagram of Human Skin Figure: Skin LayersDokumen1 halamanDermatology: Figure: Diagram of Human Skin Figure: Skin LayersAnonymous DgPsK0oQBelum ada peringkat
- 3.chap3 External Environment RobinsDokumen21 halaman3.chap3 External Environment RobinsAnonymous DgPsK0oQBelum ada peringkat
- L4 Market SegmentationDokumen7 halamanL4 Market SegmentationAnonymous DgPsK0oQBelum ada peringkat
- L3 Consumer BehaviorDokumen12 halamanL3 Consumer BehaviorAnonymous DgPsK0oQBelum ada peringkat
- L1 Principles of MarketingDokumen6 halamanL1 Principles of MarketingAnonymous DgPsK0oQBelum ada peringkat
- ProfessionalismDokumen8 halamanProfessionalismAnonymous DgPsK0oQBelum ada peringkat
- L 2 Strategic PlanningDokumen9 halamanL 2 Strategic PlanningAnonymous DgPsK0oQBelum ada peringkat
- Computer System Sevicing NC Ii: SectorDokumen44 halamanComputer System Sevicing NC Ii: SectorJess QuizzaganBelum ada peringkat
- Bs en 1991-1-5 2003 + 2009 Thermal Actions (Unsecured)Dokumen52 halamanBs en 1991-1-5 2003 + 2009 Thermal Actions (Unsecured)Tan Gui SongBelum ada peringkat
- Contemp World Module 2 Topics 1 4Dokumen95 halamanContemp World Module 2 Topics 1 4Miguel EderBelum ada peringkat
- Options Trading For Beginners Aug15 v1Dokumen187 halamanOptions Trading For Beginners Aug15 v1Glo BerriBelum ada peringkat
- WhatsNew 2019 enDokumen48 halamanWhatsNew 2019 enAdrian Martin BarrionuevoBelum ada peringkat
- Sigma Valve 2-WayDokumen2 halamanSigma Valve 2-WayRahimBelum ada peringkat
- Pie in The Sky 3Dokumen5 halamanPie in The Sky 3arsi_yaarBelum ada peringkat
- Giuliani Letter To Sen. GrahamDokumen4 halamanGiuliani Letter To Sen. GrahamFox News83% (12)
- Hoja Tecnica Item 2 DRC-9-04X12-D-H-D UV BK LSZH - F904804Q6B PDFDokumen2 halamanHoja Tecnica Item 2 DRC-9-04X12-D-H-D UV BK LSZH - F904804Q6B PDFMarco Antonio Gutierrez PulchaBelum ada peringkat
- Chapter 1 Hospital and Clinical Pharmacy Choplete PDF Notes D.Pharma 2nd Notes PDF NoteskartsDokumen7 halamanChapter 1 Hospital and Clinical Pharmacy Choplete PDF Notes D.Pharma 2nd Notes PDF NoteskartsDrx Brajendra LodhiBelum ada peringkat
- Oops in PythonDokumen64 halamanOops in PythonSyed SalmanBelum ada peringkat
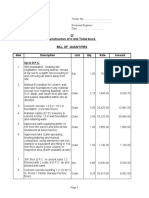
- Type BOQ For Construction of 4 Units Toilet Drawing No.04Dokumen6 halamanType BOQ For Construction of 4 Units Toilet Drawing No.04Yashika Bhathiya JayasingheBelum ada peringkat
- AN610 - Using 24lc21Dokumen9 halamanAN610 - Using 24lc21aurelioewane2022Belum ada peringkat
- People V Superior Court (Baez)Dokumen19 halamanPeople V Superior Court (Baez)Kate ChatfieldBelum ada peringkat
- ODF-2 - Learning MaterialDokumen24 halamanODF-2 - Learning MateriallevychafsBelum ada peringkat
- Key Features of A Company 1. Artificial PersonDokumen19 halamanKey Features of A Company 1. Artificial PersonVijayaragavan MBelum ada peringkat
- 7933-Article Text-35363-1-10-20230724Dokumen8 halaman7933-Article Text-35363-1-10-20230724Ridho HidayatBelum ada peringkat
- Fammthya 000001Dokumen87 halamanFammthya 000001Mohammad NorouzzadehBelum ada peringkat
- Optimization of Crude Oil DistillationDokumen8 halamanOptimization of Crude Oil DistillationJar RSBelum ada peringkat
- MDC PT ChartDokumen2 halamanMDC PT ChartKailas NimbalkarBelum ada peringkat
- จัดตารางสอบกลางภาคภาคต้น53Dokumen332 halamanจัดตารางสอบกลางภาคภาคต้น53Yuwarath SuktrakoonBelum ada peringkat
- h6811 Datadomain DsDokumen5 halamanh6811 Datadomain DsChristian EstebanBelum ada peringkat
- To The Owner / President / CeoDokumen2 halamanTo The Owner / President / CeoChriestal SorianoBelum ada peringkat
- Pyro ShieldDokumen6 halamanPyro Shieldmunim87Belum ada peringkat
- Land Degradetion NarmDokumen15 halamanLand Degradetion NarmAbdikafar Adan AbdullahiBelum ada peringkat
- Effective Communication LeaderDokumen4 halamanEffective Communication LeaderAnggun PraditaBelum ada peringkat
- 01 RFI Technical Form BiodataDokumen8 halaman01 RFI Technical Form BiodataRafiq RizkiBelum ada peringkat
- CEC Proposed Additional Canopy at Guard House (RFA-2021!09!134) (Signed 23sep21)Dokumen3 halamanCEC Proposed Additional Canopy at Guard House (RFA-2021!09!134) (Signed 23sep21)MichaelBelum ada peringkat
- Apst GraduatestageDokumen1 halamanApst Graduatestageapi-253013067Belum ada peringkat
- WPGPipingIndex Form 167 PDFDokumen201 halamanWPGPipingIndex Form 167 PDFRaj AryanBelum ada peringkat