Anda mungkin juga menyukai
- IontophoresisDokumen4 halamanIontophoresisDr GowrishankarPotturi PTBelum ada peringkat
- Anatomy and Pathoanatomic of Lumbosacral PlexusDokumen33 halamanAnatomy and Pathoanatomic of Lumbosacral PlexusRachmad FaisalBelum ada peringkat
- Vitiligo PPT (1) .PPTX LectureDokumen35 halamanVitiligo PPT (1) .PPTX LectureVinay DhranaBelum ada peringkat
- HeliotherapyDokumen20 halamanHeliotherapyDodo JuniorBelum ada peringkat
- Peripheral Nerve InjuriesDokumen25 halamanPeripheral Nerve InjuriesaboujisBelum ada peringkat
- Brachial Plexus InjuryDokumen21 halamanBrachial Plexus InjurySemi IqbalBelum ada peringkat
- Rebox ElectrotherapyDokumen2 halamanRebox Electrotherapyakheel ahammedBelum ada peringkat
- Infrared Radiation Therapy: By: Vikalp Mohan Saxena Roll No.: 29 B.P.T 2 YearDokumen9 halamanInfrared Radiation Therapy: By: Vikalp Mohan Saxena Roll No.: 29 B.P.T 2 YearApoorvBelum ada peringkat
- Muscle Plasticity in Response To Electrical Stimulation: - Priyanka. Parate MPTH, PuneDokumen35 halamanMuscle Plasticity in Response To Electrical Stimulation: - Priyanka. Parate MPTH, Punemilananand100% (1)
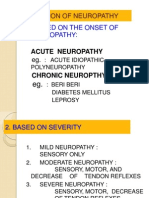
- Classification of NeuropathyDokumen16 halamanClassification of NeuropathysekiannBelum ada peringkat
- Electrotherapy: DR Ramaiah Choudhary PhysiotherapistDokumen13 halamanElectrotherapy: DR Ramaiah Choudhary Physiotherapistvenkata ramakrishnaiahBelum ada peringkat
- Overview of Spinal Cord Injuries - PhysiopediaDokumen20 halamanOverview of Spinal Cord Injuries - PhysiopediaRaina Ginella DsouzaBelum ada peringkat
- Basics of Electrotherapy 2nd PDFDokumen175 halamanBasics of Electrotherapy 2nd PDFPraneetha NouduriBelum ada peringkat
- Cranial NeuropathiesDokumen74 halamanCranial NeuropathiesKevin Woodard100% (1)
- Ataxias Neuro Condition DetailedDokumen80 halamanAtaxias Neuro Condition DetailedMikail AtiyehBelum ada peringkat
- Muscle SpindlesDokumen19 halamanMuscle SpindlesBenedek IldikoBelum ada peringkat
- Final Coma StimulationDokumen23 halamanFinal Coma StimulationpreetisagarBelum ada peringkat
- Receptor PhysiologyDokumen34 halamanReceptor PhysiologyKarl Torres Uganiza RmtBelum ada peringkat
- Internal CapsuleDokumen25 halamanInternal CapsuleMadan KumarBelum ada peringkat
- Therapybook Interferencial TherapyDokumen34 halamanTherapybook Interferencial TherapyBrian RaymondBelum ada peringkat
- Module 1 - NeuropsychologyDokumen4 halamanModule 1 - Neuropsychologyaysha farihaBelum ada peringkat
- Physiotherapy-IInd YrDokumen10 halamanPhysiotherapy-IInd YrEashwar Prasad Meenakshi100% (1)
- Biomechanics of Peripheral and Spinal Nerve RootsDokumen86 halamanBiomechanics of Peripheral and Spinal Nerve RootsJawad HassanBelum ada peringkat
- Corticospinal Tract Pyramidal Tract - PhysiopediaDokumen4 halamanCorticospinal Tract Pyramidal Tract - PhysiopediaNrs Sani Sule MashiBelum ada peringkat
- Dysphagia ManagementDokumen21 halamanDysphagia ManagementSooraj A. O.100% (1)
- Lung SurgeriesDokumen43 halamanLung SurgeriesSereinBelum ada peringkat
- Motor Neuron DiseaseDokumen8 halamanMotor Neuron DiseaseyigoBelum ada peringkat
- Faradic CurrentDokumen13 halamanFaradic CurrentArun Tamilvanan0% (1)
- Foundation Handout For Physical Therapy Students in OLFUDokumen3 halamanFoundation Handout For Physical Therapy Students in OLFUBogart Macatangay100% (1)
- Brachial Plexus InjuriesDokumen64 halamanBrachial Plexus Injuriesprashanth naikBelum ada peringkat
- Bicipital TendonitisDokumen2 halamanBicipital TendonitisJ Cheung100% (2)
- Foot DropDokumen64 halamanFoot DropRam Chandra Reddy100% (1)
- Tx3: Bobath'S Neurodevelopmental Treatment: PT Applications Team DLSMHSI CRS PT Department AY 2018-2019Dokumen4 halamanTx3: Bobath'S Neurodevelopmental Treatment: PT Applications Team DLSMHSI CRS PT Department AY 2018-2019Pauline JaleaBelum ada peringkat
- Transverse MyelitisDokumen19 halamanTransverse MyelitisAnonymous YHQmN8a01100% (1)
- Faradic Foot BathDokumen16 halamanFaradic Foot BathMaansi Gupta100% (1)
- Articular Neurophysiology: Presented by - Yogesh VyasDokumen15 halamanArticular Neurophysiology: Presented by - Yogesh VyasvictoryvelavaBelum ada peringkat
- Myasthenia Gravis BrochureDokumen2 halamanMyasthenia Gravis BrochureMolly100% (1)
- Short Wave DiathermyDokumen6 halamanShort Wave DiathermyMayakkannan A VBelum ada peringkat
- Carpal Tunnel SyndromeDokumen2 halamanCarpal Tunnel Syndromeurkevet100% (1)
- Vojta Therapy: Reflex Creeping in A Prone Lying Position and Reflex Rolling From A Supine and Side LyingDokumen7 halamanVojta Therapy: Reflex Creeping in A Prone Lying Position and Reflex Rolling From A Supine and Side LyingSonali SoumyashreeBelum ada peringkat
- Rehabilitation Engineering Fact Sheet PDFDokumen2 halamanRehabilitation Engineering Fact Sheet PDFYahya AlkamaliBelum ada peringkat
- CP PDFDokumen7 halamanCP PDFannaBelum ada peringkat
- McKenzie CONCEPT AnilDokumen12 halamanMcKenzie CONCEPT AnilSOUMYADEEP BHUINYABelum ada peringkat
- Peripheral Nerve InjuriesDokumen12 halamanPeripheral Nerve InjuriesJiggs LimBelum ada peringkat
- Fundamental and Derived PositionDokumen47 halamanFundamental and Derived PositionAmbusam Anita100% (1)
- Sample Chapter 7 Therapeutic Mod Ali TiesDokumen28 halamanSample Chapter 7 Therapeutic Mod Ali Tiesmdarif4ptBelum ada peringkat
- Students Clinical Case AnalysisDokumen5 halamanStudents Clinical Case Analysisjacc_282Belum ada peringkat
- Introduction To Functional Electrical StimulationDokumen14 halamanIntroduction To Functional Electrical StimulationJia HuiBelum ada peringkat
- MUHS - BPT - 2017 - 4 - Winter - B.P.TH - 51411 Musculoskeletal PhysiotherapyDokumen2 halamanMUHS - BPT - 2017 - 4 - Winter - B.P.TH - 51411 Musculoskeletal PhysiotherapyYuvraj AtholeBelum ada peringkat
- Tabes Dorsalis: Primary Stage: After The Initial InfectionDokumen3 halamanTabes Dorsalis: Primary Stage: After The Initial InfectionsekarananyaBelum ada peringkat
- Chapter # 4: Physical Assessment As A Screening ToolDokumen89 halamanChapter # 4: Physical Assessment As A Screening Toolmuhammad awaisBelum ada peringkat
- Causal GiaDokumen22 halamanCausal GiaAmitBelum ada peringkat
- Motor Neuron Disease.Dokumen38 halamanMotor Neuron Disease.sanjana sangleBelum ada peringkat
- Neuro-Coordination Umair PTDokumen20 halamanNeuro-Coordination Umair PTFatima SeharBelum ada peringkat
- Amyotrophic Lateral SclerosisDokumen15 halamanAmyotrophic Lateral SclerosisYakan AbdulrahmanBelum ada peringkat
- Balance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementDari EverandBalance Dysfunction in Parkinson’s Disease: Basic Mechanisms to Clinical ManagementBelum ada peringkat
- K5 - Disorders of Autonomic Nervous SystemDokumen47 halamanK5 - Disorders of Autonomic Nervous Systemengkiii100% (1)
- ANS SpinalcordDokumen23 halamanANS SpinalcordJay FickleBelum ada peringkat
- Lecture 9Dokumen13 halamanLecture 9bakuBelum ada peringkat
- Headache Kuliah New1 PDFDokumen59 halamanHeadache Kuliah New1 PDFDenis Harli SiregarBelum ada peringkat
- Abstrak English Kak MeiDokumen1 halamanAbstrak English Kak MeiDenis Harli SiregarBelum ada peringkat
- Spinal Cord InjuryDokumen97 halamanSpinal Cord Injuryamoon1275% (4)
- Long Term Functional Outcome in Hemispherectomy ChildrenDokumen21 halamanLong Term Functional Outcome in Hemispherectomy ChildrenDenis Harli SiregarBelum ada peringkat
- Relationship of Childhood Headache With Preferences in LeisureDokumen30 halamanRelationship of Childhood Headache With Preferences in LeisureDenis Harli SiregarBelum ada peringkat
- PD DSM 4 Vs 5Dokumen15 halamanPD DSM 4 Vs 5satish2k3Belum ada peringkat
- Cephalagia 2015 - p527 PDFDokumen11 halamanCephalagia 2015 - p527 PDFDenis Harli SiregarBelum ada peringkat
- Stroke PreventionDokumen69 halamanStroke PreventionDenis Harli SiregarBelum ada peringkat
- Dementia GuidelineDokumen2 halamanDementia Guideline-Timothy Osho-Belum ada peringkat
- Atrial Fibrillation, Cognitive Decline and DementiaDokumen33 halamanAtrial Fibrillation, Cognitive Decline and DementiaDenis Harli SiregarBelum ada peringkat
- DR - Syafrizal NST, SP - PDDokumen69 halamanDR - Syafrizal NST, SP - PDDenis Harli SiregarBelum ada peringkat
- Dr. Dharma LindartoDokumen55 halamanDr. Dharma LindartoDenis Harli Siregar100% (1)
- Guidelines PresentationDokumen22 halamanGuidelines PresentationDenis Harli SiregarBelum ada peringkat
- Hyper Guidelines 2011Dokumen65 halamanHyper Guidelines 2011wrocha2000Belum ada peringkat
- Cataract, Conjunctivitis, DRDokumen62 halamanCataract, Conjunctivitis, DRDenis Harli SiregarBelum ada peringkat
- Downloadfile 66Dokumen7 halamanDownloadfile 66Denis Harli SiregarBelum ada peringkat
- Cerebral Venous ThrombosisDokumen20 halamanCerebral Venous ThrombosisDenis Harli SiregarBelum ada peringkat
- Lyme Disease PDFDokumen47 halamanLyme Disease PDFDenis Harli SiregarBelum ada peringkat
- Neurology 2007 - p1002Dokumen6 halamanNeurology 2007 - p1002Denis Harli SiregarBelum ada peringkat
- Wilmot DKK, 2006Dokumen8 halamanWilmot DKK, 2006Denis Harli SiregarBelum ada peringkat
- Recent Advances of Tuberculous Meningitis TherapyDokumen45 halamanRecent Advances of Tuberculous Meningitis TherapyDenis Harli SiregarBelum ada peringkat
- Biochemistry The Chemical Reactions of Living Cells 2d Ed Vols 1 2 David E. MetzlerDokumen1.977 halamanBiochemistry The Chemical Reactions of Living Cells 2d Ed Vols 1 2 David E. MetzlerEvelyn Biscari100% (7)
- Laporan Pasien Neurologi Rumah Sakit Kesdam Bukit Barisan Medan PERIODE 9 - 15 JUNI 2015Dokumen3 halamanLaporan Pasien Neurologi Rumah Sakit Kesdam Bukit Barisan Medan PERIODE 9 - 15 JUNI 2015Denis Harli SiregarBelum ada peringkat
- 1Dokumen15 halaman1Ceejhay LeeBelum ada peringkat
- Downloaded File 79Dokumen11 halamanDownloaded File 79Denis Harli SiregarBelum ada peringkat
- Bolus Dose Nicardipine PDFDokumen28 halamanBolus Dose Nicardipine PDFDenis Harli SiregarBelum ada peringkat
- Spinal Cord InjuriesDokumen51 halamanSpinal Cord Injurieswanglee2000Belum ada peringkat
- Neurorehabilitation ArticleDokumen7 halamanNeurorehabilitation ArticleDenis Harli SiregarBelum ada peringkat
- Gardens Illustrated FernandoDokumen4 halamanGardens Illustrated FernandoMariaBelum ada peringkat
- LEGO Group A Strategic and Valuation AnalysisDokumen85 halamanLEGO Group A Strategic and Valuation AnalysisRudmila Ahmed50% (2)
- Part 1Dokumen14 halamanPart 1Jat SardanBelum ada peringkat
- Project Definition and DescriptionDokumen9 halamanProject Definition and DescriptionEileen VelasquezBelum ada peringkat
- Class XI Economics 2011Dokumen159 halamanClass XI Economics 2011Ramita Udayashankar0% (1)
- MSDS Blattanex GelDokumen5 halamanMSDS Blattanex GelSadhana SentosaBelum ada peringkat
- Presentation Airbnb ProfileDokumen14 halamanPresentation Airbnb ProfileGuillermo VillacrésBelum ada peringkat
- National Geographic Traveller India - July 2016-P2PDokumen104 halamanNational Geographic Traveller India - July 2016-P2PPeter100% (2)
- What Is Degrowth - Demaria Schneider Sekulova Martinez Alier Env ValuesDokumen27 halamanWhat Is Degrowth - Demaria Schneider Sekulova Martinez Alier Env ValuesNayara SantosBelum ada peringkat
- 2 - (Accounting For Foreign Currency Transaction)Dokumen25 halaman2 - (Accounting For Foreign Currency Transaction)Stephiel SumpBelum ada peringkat
- IO RE 04 Distance Learning Module and WorksheetDokumen21 halamanIO RE 04 Distance Learning Module and WorksheetVince Bryan San PabloBelum ada peringkat
- Global Supply Chain Top 25 Report 2021Dokumen19 halamanGlobal Supply Chain Top 25 Report 2021ImportclickBelum ada peringkat
- Learning Activity 5.2 Concept ReviewDokumen4 halamanLearning Activity 5.2 Concept ReviewJames CantorneBelum ada peringkat
- CV - Cover LetterDokumen2 halamanCV - Cover LetterMoutagaBelum ada peringkat
- Astm A709-04Dokumen8 halamanAstm A709-04Артем ТитовBelum ada peringkat
- Third Party Intervention in The Criminal TrialDokumen8 halamanThird Party Intervention in The Criminal TrialVenkat Raman JBelum ada peringkat
- Assignment 2 Format Baru 17042011Dokumen8 halamanAssignment 2 Format Baru 17042011Noor Zilawati SabtuBelum ada peringkat
- Business Research Chapter 1Dokumen27 halamanBusiness Research Chapter 1Toto H. Ali100% (2)
- TLE ICT CY9 w4 PDFDokumen5 halamanTLE ICT CY9 w4 PDFMichelle DaurogBelum ada peringkat
- AgrippaDokumen4 halamanAgrippaFloorkitBelum ada peringkat
- RBConcept Universal Instruction ManualDokumen19 halamanRBConcept Universal Instruction Manualyan henrique primaoBelum ada peringkat
- FINS1612 Capital Markets and Institutions S12016Dokumen15 halamanFINS1612 Capital Markets and Institutions S12016fakableBelum ada peringkat
- Labor Law Highlights, 1915-2015: Labor Review Has Been in Publication. All The LegislationDokumen13 halamanLabor Law Highlights, 1915-2015: Labor Review Has Been in Publication. All The LegislationIgu jumaBelum ada peringkat
- Dental CeramicsDokumen6 halamanDental CeramicsDeema FlembanBelum ada peringkat
- Chapter 4 Lesson ProperDokumen44 halamanChapter 4 Lesson ProperWenceslao LynBelum ada peringkat
- The City of GodDokumen16 halamanThe City of GodJei Em MonteflorBelum ada peringkat
- CONCEPTUAL LITERATURE (Chapter 2)Dokumen2 halamanCONCEPTUAL LITERATURE (Chapter 2)lilibeth garciaBelum ada peringkat
- Strama-Ayala Land, Inc.Dokumen5 halamanStrama-Ayala Land, Inc.Akako MatsumotoBelum ada peringkat
- World Price List 2014: Adventys Induction Counter TopsDokumen4 halamanWorld Price List 2014: Adventys Induction Counter TopsdiogocorollaBelum ada peringkat
- On Evil - Terry EagletonDokumen44 halamanOn Evil - Terry EagletonconelcaballocansadoBelum ada peringkat