Anda mungkin juga menyukai
- 1dental Needs and Dental DemandsDokumen31 halaman1dental Needs and Dental DemandsYasminBelum ada peringkat
- Pediatric Dentistry: Fourth EditionDokumen6 halamanPediatric Dentistry: Fourth EditionFadiaBelum ada peringkat
- Essential Tissue Healing of the Face and NeckDari EverandEssential Tissue Healing of the Face and NeckPenilaian: 5 dari 5 bintang5/5 (2)
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideDari EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideBelum ada peringkat
- Pediatric Oral HealthDokumen172 halamanPediatric Oral HealthArif HidayatBelum ada peringkat
- Pediatric Dentistry.Dokumen20 halamanPediatric Dentistry.Patra PrimadanaBelum ada peringkat
- Dental Trauma Professional PamphletDokumen3 halamanDental Trauma Professional Pamphletnona aryan50% (2)
- Tooth Discolour at Ion PedoDokumen28 halamanTooth Discolour at Ion PedoFourthMolar.comBelum ada peringkat
- Traumatic InjuriesDokumen43 halamanTraumatic Injuriessandsiramesh100% (1)
- Management of Fear Anxiety PedoDokumen21 halamanManagement of Fear Anxiety PedoFourthMolar.comBelum ada peringkat
- Anatomy and Physiology of Teeth and Oral CavityDokumen4 halamanAnatomy and Physiology of Teeth and Oral CavityVillanz Vimal ChanderBelum ada peringkat
- Epidemiologi Dental CariesDokumen21 halamanEpidemiologi Dental CariesSampahAjaBelum ada peringkat
- Single Vs Multiple Visits in PulpectomyDokumen7 halamanSingle Vs Multiple Visits in PulpectomyHudh HudBelum ada peringkat
- DR Neeraj Gugnani - Ecc PDFDokumen29 halamanDR Neeraj Gugnani - Ecc PDFshailaja chintaBelum ada peringkat
- Headches and Facial PainDokumen33 halamanHeadches and Facial PainIsak ShatikaBelum ada peringkat
- Role of A Pedodontist in Cleft Lip and Cleft Palate Rehabilitation - An OverviewDokumen25 halamanRole of A Pedodontist in Cleft Lip and Cleft Palate Rehabilitation - An OverviewIJAR JOURNALBelum ada peringkat
- Conscious Sedation Oral SurgeryDokumen21 halamanConscious Sedation Oral SurgeryFourthMolar.comBelum ada peringkat
- Chapter 41.Ppt HypersensitivityDokumen63 halamanChapter 41.Ppt HypersensitivityMaria Mercedes LeivaBelum ada peringkat
- Dental Radiography For The Pediatric Patient PedoDokumen30 halamanDental Radiography For The Pediatric Patient PedoFourthMolar.comBelum ada peringkat
- DR Nick Lekic - Space MaintainersDokumen35 halamanDR Nick Lekic - Space MaintainersanatomimanusiaBelum ada peringkat
- Presentation1 140115092530 Phpapp02Dokumen131 halamanPresentation1 140115092530 Phpapp02Ana LucaBelum ada peringkat
- 1st Course Introductory Course in Paediatric Dentistry&Childhood StagesDokumen29 halaman1st Course Introductory Course in Paediatric Dentistry&Childhood StagesChristosSougkakisBelum ada peringkat
- Early Chilhood CariesDokumen45 halamanEarly Chilhood CariesAnn Ezzat100% (2)
- Regenerative Endodontics Barriers and Strategies For Clinical Translation 2012 Dental Clinics of North AmericaDokumen11 halamanRegenerative Endodontics Barriers and Strategies For Clinical Translation 2012 Dental Clinics of North AmericaCaioSelaimenBelum ada peringkat
- Case Report: M E C C C S AC RDokumen3 halamanCase Report: M E C C C S AC RRaja Dean Collin SiagianBelum ada peringkat
- Pediatric DentistryDokumen15 halamanPediatric Dentistrymirfanulhaq100% (2)
- Pharmacological Behaviour Management (Quite Fine) (Nellore)Dokumen82 halamanPharmacological Behaviour Management (Quite Fine) (Nellore)ultraswamy50% (2)
- What Is EBD?Dokumen7 halamanWhat Is EBD?RATHEESH M. S.Belum ada peringkat
- Early Childhood Caries - A Review PDFDokumen7 halamanEarly Childhood Caries - A Review PDFdr parveen bathlaBelum ada peringkat
- Crown in Pediatric DentistryDokumen85 halamanCrown in Pediatric DentistryBhawna SaxenaBelum ada peringkat
- Calculate The Max Doses of Local Anesthesia in DentistryDokumen13 halamanCalculate The Max Doses of Local Anesthesia in DentistryYasser MagramiBelum ada peringkat
- Dental Anxiety - FullDokumen14 halamanDental Anxiety - FullTJPRC PublicationsBelum ada peringkat
- Vital Pulp Therapy in Primary TeethDokumen10 halamanVital Pulp Therapy in Primary Teethyuni madjidBelum ada peringkat
- Concious Sedation PedoDokumen29 halamanConcious Sedation PedodrkameshBelum ada peringkat
- Adpied Paper From EmailDokumen17 halamanAdpied Paper From Emailapi-401213596Belum ada peringkat
- Minor Oral Surgical Procedures in Children ClassDokumen65 halamanMinor Oral Surgical Procedures in Children ClassReenaChauhanBelum ada peringkat
- Infant Oral Health CareDokumen16 halamanInfant Oral Health CareAJPEDO LIFE100% (1)
- Local Anesthesia in Peadiatric Dentistry: Presented By: DR - Walija Ansari & Dr. Yousuf Ahmed KhanDokumen24 halamanLocal Anesthesia in Peadiatric Dentistry: Presented By: DR - Walija Ansari & Dr. Yousuf Ahmed KhanChaudhry Abdullah DeuBelum ada peringkat
- Dental HygieneDokumen3 halamanDental Hygieneapi-507354264Belum ada peringkat
- Pediatric Nutrition and Nutritional Disorders: DR Ibraahim Guled MBCHB, Mmed (Paediatrics)Dokumen74 halamanPediatric Nutrition and Nutritional Disorders: DR Ibraahim Guled MBCHB, Mmed (Paediatrics)Mohamed AliBelum ada peringkat
- Pediatric DentistryDokumen15 halamanPediatric DentistryPeyman Dhg100% (2)
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDokumen39 halamanAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyBelum ada peringkat
- Child PsychologyDokumen35 halamanChild PsychologyAmit Gaur0% (1)
- SSCDokumen50 halamanSSCMustafa Tambawala100% (1)
- Department of Pediatrics and Preventive Dentistry.: Local Anasthesia in Pediatric DentistryDokumen27 halamanDepartment of Pediatrics and Preventive Dentistry.: Local Anasthesia in Pediatric DentistrySudip Chakraborty100% (1)
- Dental Anatomy and PhysiologyDokumen36 halamanDental Anatomy and PhysiologyCpt.WnchstrBelum ada peringkat
- EccDokumen60 halamanEccLoo Ying YingBelum ada peringkat
- Pulp Therapy For Primary and Immature Permanent TeethDokumen11 halamanPulp Therapy For Primary and Immature Permanent TeethPrabhjot KaurBelum ada peringkat
- Department of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearDokumen29 halamanDepartment of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearFarzana ShereenBelum ada peringkat
- Management of Traumatic Injuries To Primary Young Permanent Teeth PedoDokumen142 halamanManagement of Traumatic Injuries To Primary Young Permanent Teeth PedoFourthMolar.comBelum ada peringkat
- Non-Caries Dental DiseaseDokumen61 halamanNon-Caries Dental Diseaseapi-19916399Belum ada peringkat
- Dental HipersensitivityDokumen28 halamanDental HipersensitivitySergio KancyperBelum ada peringkat
- TMJ AnatomiDokumen53 halamanTMJ AnatomiNiTa DöéMy HarDianaBelum ada peringkat
- "Etiology of Malocclusion": Hemam Shankar SinghDokumen63 halaman"Etiology of Malocclusion": Hemam Shankar SinghMira Anggriani50% (2)
- RCDSO Guidelines Implant DentistryDokumen16 halamanRCDSO Guidelines Implant DentistrydoctorlupuBelum ada peringkat
- Management of Medically Compromised Orthodontic PatientsDokumen64 halamanManagement of Medically Compromised Orthodontic Patientsakshi1947Belum ada peringkat
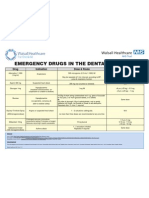
- Emergency Drugs Poster - Layout 1 in Dental PracticeDokumen1 halamanEmergency Drugs Poster - Layout 1 in Dental PracticeFady AtefBelum ada peringkat
- Manual CariogramDokumen51 halamanManual CariogramDesty DarmaBelum ada peringkat
- Child in The Dental ClinicDokumen28 halamanChild in The Dental ClinicZozoBelum ada peringkat
- Shoulder Pain in Hemiplegia: Statistical Relationship With Five VariablesDokumen3 halamanShoulder Pain in Hemiplegia: Statistical Relationship With Five VariablesSahithya MBelum ada peringkat
- Filipino Health PracticesDokumen2 halamanFilipino Health PracticesheeBelum ada peringkat
- Normal Reçete İle Verilmesi Gereken İzlemeye Tabi İlaç ListesiDokumen4 halamanNormal Reçete İle Verilmesi Gereken İzlemeye Tabi İlaç ListesicanankeBelum ada peringkat
- OsteoarthritisDokumen386 halamanOsteoarthritisA Syed ZahidBelum ada peringkat
- USDA Pain ClassificationDokumen2 halamanUSDA Pain ClassificationnbcdserBelum ada peringkat
- Abbott 2018Dokumen15 halamanAbbott 2018Shriya ShahuBelum ada peringkat
- Medications Exercise/Activity Treatment Health Teachings Outpatient Diet Spiritual CareDokumen1 halamanMedications Exercise/Activity Treatment Health Teachings Outpatient Diet Spiritual Carelalaine nadulpitBelum ada peringkat
- 0-10 Pain Scale1Dokumen1 halaman0-10 Pain Scale1Ruli Syukran MaulanaBelum ada peringkat
- Campbell and Others V WhylieDokumen11 halamanCampbell and Others V WhylieShaniel T HunterBelum ada peringkat
- Nursing Diagnoses Arranged by GordonDokumen9 halamanNursing Diagnoses Arranged by GordonJoedeson Aroco BungubungBelum ada peringkat
- Home Massage-Transforming Family Life Through The Healing Power of TouchDokumen209 halamanHome Massage-Transforming Family Life Through The Healing Power of TouchYudhi FaisalBelum ada peringkat
- (MEGAPOST) MACAVITY IMP Overcoming Your Emotional Issues - Attain Emotional Health, Self-Esteem, Inner Game & Well-Being PDFDokumen28 halaman(MEGAPOST) MACAVITY IMP Overcoming Your Emotional Issues - Attain Emotional Health, Self-Esteem, Inner Game & Well-Being PDFNik AHBelum ada peringkat
- ProActive Training Case Study 4Dokumen8 halamanProActive Training Case Study 4danthemanyvrBelum ada peringkat
- Endorphins HandoutDokumen1 halamanEndorphins Handoutapi-260339450Belum ada peringkat
- HAAD Exam For Nurses Questions 2018Dokumen46 halamanHAAD Exam For Nurses Questions 2018Asif Newaz100% (6)
- 1 s2.0 S1529943016309226 MainDokumen6 halaman1 s2.0 S1529943016309226 Mainhakan sonsuzlukluBelum ada peringkat
- Proceeding of The LAVC Latin American Veterinary Conference Apr. 22-25, 2014 - Lima, PeruDokumen3 halamanProceeding of The LAVC Latin American Veterinary Conference Apr. 22-25, 2014 - Lima, PeruLove GeckoBelum ada peringkat
- LECTURE 8 - Clinical Assessment-F17-4610 PDFDokumen21 halamanLECTURE 8 - Clinical Assessment-F17-4610 PDFJon DoeBelum ada peringkat
- PANACEA Leomicio Offemaria CorpuzDokumen2 halamanPANACEA Leomicio Offemaria CorpuzNikki RiveraBelum ada peringkat
- Nursing Care PlanDokumen3 halamanNursing Care PlanJoyce AnglubenBelum ada peringkat
- Bioptron Biology 1Dokumen6 halamanBioptron Biology 1Nick100% (1)
- EMD Guidecards PDFDokumen49 halamanEMD Guidecards PDFЛизатро1980 ЛизаBelum ada peringkat
- Pediatrics Nursing L5Dokumen89 halamanPediatrics Nursing L5MaxBelum ada peringkat
- Facet Joint Pain-Advances in Patient Selection and TreatmentDokumen16 halamanFacet Joint Pain-Advances in Patient Selection and TreatmentthiagoBelum ada peringkat
- Indian Journal of Applied Basic Medical Science Jan 2011Dokumen112 halamanIndian Journal of Applied Basic Medical Science Jan 2011Soham AnandBelum ada peringkat
- Nursing DiagnosisDokumen1 halamanNursing DiagnosisTahlia FrancisBelum ada peringkat
- 1.12 Management of Control Impairment HandoutDokumen9 halaman1.12 Management of Control Impairment Handoutmansigupta88Belum ada peringkat
- ARTHRITISrevieweditedDokumen26 halamanARTHRITISrevieweditedFelix Morales PerezBelum ada peringkat
- Thalhamer 2017 Critique FDMDokumen6 halamanThalhamer 2017 Critique FDMArthurBelum ada peringkat
- Mcgraw-Hill Companies, IncDokumen2 halamanMcgraw-Hill Companies, IncLu LubNaBelum ada peringkat