Anda mungkin juga menyukai
- A Pocket Guide To Blood Pressure Measurement in ChildrenDokumen4 halamanA Pocket Guide To Blood Pressure Measurement in ChildrenKira23406Belum ada peringkat
- Retropharyngeal Abscess ReportDokumen49 halamanRetropharyngeal Abscess ReportAyen FornollesBelum ada peringkat
- Functional DyspepsiaDokumen4 halamanFunctional DyspepsiaEasy Orient DewantariBelum ada peringkat
- Drug-Induced Movement Disorders GuideDokumen136 halamanDrug-Induced Movement Disorders GuideYamini DevendranBelum ada peringkat
- Neurological Eval SensoryDokumen25 halamanNeurological Eval SensoryAyen FornollesBelum ada peringkat
- Basic ECG Interpretation - LeonardDokumen33 halamanBasic ECG Interpretation - LeonardAyen FornollesBelum ada peringkat
- Case Report FinalDokumen21 halamanCase Report FinalAyen FornollesBelum ada peringkat
- Autism Spectrum Disorder and AdhdDokumen1 halamanAutism Spectrum Disorder and AdhdAyen FornollesBelum ada peringkat
- CPG AID - Pocket Guide.v7 PDFDokumen31 halamanCPG AID - Pocket Guide.v7 PDFR ParkBelum ada peringkat
- Pidsp Covid Guidelines 02.06.2021Dokumen77 halamanPidsp Covid Guidelines 02.06.2021Sheena PasionBelum ada peringkat
- NTP MOP 6th Edition PDFDokumen192 halamanNTP MOP 6th Edition PDFZai Ra DianaBelum ada peringkat
- Childhood Immunization Part Ii: Roxanne Jeen L. FornollesDokumen8 halamanChildhood Immunization Part Ii: Roxanne Jeen L. FornollesAyen FornollesBelum ada peringkat
- Practice Guidelines For Obstetric Anesthesia PDFDokumen31 halamanPractice Guidelines For Obstetric Anesthesia PDFLiviliaMiftaBelum ada peringkat
- ILAE Clasiffication and Teminology 2017Dokumen10 halamanILAE Clasiffication and Teminology 2017Prabaningrum DwidjoasmoroBelum ada peringkat
- WHO 2019 nCoV Clinical 2021.1 EngDokumen81 halamanWHO 2019 nCoV Clinical 2021.1 EngAmjad Ali AfridiBelum ada peringkat
- Abnormal Uterine Bleeding in AdolescentsDokumen40 halamanAbnormal Uterine Bleeding in AdolescentsAyen FornollesBelum ada peringkat
- General Data: - J.C - 12 Yrs Old/ M - Filipino - RC - Mandaue City - 1 Admission in UcmedDokumen23 halamanGeneral Data: - J.C - 12 Yrs Old/ M - Filipino - RC - Mandaue City - 1 Admission in UcmedAyen FornollesBelum ada peringkat
- Related Protocols / Related Links Include:: Lumbar Puncture in The NeonateDokumen7 halamanRelated Protocols / Related Links Include:: Lumbar Puncture in The NeonateAyen FornollesBelum ada peringkat
- Toxic Liver DiseaseDokumen28 halamanToxic Liver DiseaseAyen FornollesBelum ada peringkat
- Recurrent TonsilitisDokumen16 halamanRecurrent TonsilitisAyen FornollesBelum ada peringkat
- APRIL MORBIDITY AND MORTALITY CASE CONFERENCE: KAWASAKI DISEASEDokumen30 halamanAPRIL MORBIDITY AND MORTALITY CASE CONFERENCE: KAWASAKI DISEASEAyen FornollesBelum ada peringkat
- Neurological Exam Lecture NotesDokumen26 halamanNeurological Exam Lecture NotesNaveen KovalBelum ada peringkat
- General Data and Chief ComplaintDokumen21 halamanGeneral Data and Chief ComplaintAyen FornollesBelum ada peringkat
- Hyperbil ABO IncompDokumen9 halamanHyperbil ABO IncompAyen FornollesBelum ada peringkat
- Recurrent TonsilitisDokumen16 halamanRecurrent TonsilitisAyen FornollesBelum ada peringkat
- Hyperbil ABO IncompDokumen9 halamanHyperbil ABO IncompAyen FornollesBelum ada peringkat
- TB Meningitis Masquerades as Migraine in TeenDokumen75 halamanTB Meningitis Masquerades as Migraine in TeenAyen FornollesBelum ada peringkat
- M&m-Hypovolemic ShockDokumen29 halamanM&m-Hypovolemic ShockAyen FornollesBelum ada peringkat
- Prophylactic Administration of Ondansetron inDokumen16 halamanProphylactic Administration of Ondansetron inRyan FornollesBelum ada peringkat
- Nelson's Club - AtelectasisDokumen22 halamanNelson's Club - AtelectasisAyen FornollesBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Aesculap Basic Sets of Neurosurgical Instruments PDFDokumen10 halamanAesculap Basic Sets of Neurosurgical Instruments PDFyudiBelum ada peringkat
- OMM Review SheetDokumen9 halamanOMM Review SheetSolomon Seth Sallfors100% (2)
- Cummings 2001Dokumen7 halamanCummings 2001Gopi KrishnanBelum ada peringkat
- Monitorizarea Cardiaca Recunoasterea RitmurilorDokumen378 halamanMonitorizarea Cardiaca Recunoasterea Ritmurilorsun seal100% (1)
- Psychosocial AspectsDokumen26 halamanPsychosocial AspectsAyn BedoniaBelum ada peringkat
- Uss Features of Iugr and Macrosomia.Dokumen11 halamanUss Features of Iugr and Macrosomia.ibmreadywriterBelum ada peringkat
- Any ScanDokumen28 halamanAny ScanSergeyKuznetsovBelum ada peringkat
- ICAP Basic ICRA With MatrixDokumen4 halamanICAP Basic ICRA With MatrixmiptahulBelum ada peringkat
- Plan of The Course Anatomy and Clinical Anatomy: Academic Year 2013/2014Dokumen7 halamanPlan of The Course Anatomy and Clinical Anatomy: Academic Year 2013/2014Rinor MujajBelum ada peringkat
- Colgate Transcend Case Brief KidsDokumen6 halamanColgate Transcend Case Brief KidsRohit GuptaBelum ada peringkat
- Sun Pharma IR PresentationDokumen56 halamanSun Pharma IR PresentationAishwarya MauryaBelum ada peringkat
- Paediatric Antibiotic TeddyDokumen1 halamanPaediatric Antibiotic Teddyayu fitrianiBelum ada peringkat
- Current Immunization Schedule of Routine Epi in PakistanDokumen2 halamanCurrent Immunization Schedule of Routine Epi in PakistanDilawar JanBelum ada peringkat
- FasciaDokumen53 halamanFasciaGustavo CabanasBelum ada peringkat
- Acute Abdomen, Nyeri Akut AbdomenDokumen35 halamanAcute Abdomen, Nyeri Akut AbdomenYanuar Yudha SudrajatBelum ada peringkat
- Chloride The Queen of ElectrolytesDokumen9 halamanChloride The Queen of ElectrolytesYancy Erazo DoradoBelum ada peringkat
- LIFE Kite Flying Sponsorship LetterDokumen3 halamanLIFE Kite Flying Sponsorship LetterMarjorie CuaBelum ada peringkat
- Prospectus Ph.D. July 2021 SessionDokumen5 halamanProspectus Ph.D. July 2021 SessiondamadolBelum ada peringkat
- PROFILE of Virk HospitalDokumen14 halamanPROFILE of Virk HospitalwittyvishwasBelum ada peringkat
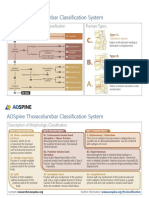
- AOSpine Thoracolumbar Classification System - Pocket CardDokumen2 halamanAOSpine Thoracolumbar Classification System - Pocket CardFernanda Ahumada0% (1)
- Checklist For BabyDokumen5 halamanChecklist For BabysgrandeaBelum ada peringkat
- Avascular NecrosisDokumen41 halamanAvascular NecrosisMohd Johari Mohd Shafuwan100% (1)
- ITLS 8e Advanced Pre-Test - Annotated Key PDFDokumen10 halamanITLS 8e Advanced Pre-Test - Annotated Key PDFJohn E. Ibrahim100% (1)
- Contact DermatitisDokumen11 halamanContact Dermatitismits98Belum ada peringkat
- Current Concepts: Scapular Dyskinesis: W Ben Kibler, Aaron SciasciaDokumen7 halamanCurrent Concepts: Scapular Dyskinesis: W Ben Kibler, Aaron SciasciatomxtchBelum ada peringkat
- Postural, DrainageDokumen7 halamanPostural, DrainageJames ThompsonBelum ada peringkat
- Mongtu Ngo ResumeDokumen1 halamanMongtu Ngo ResumeKrissy NgoBelum ada peringkat
- Phyto PharmacologyDokumen56 halamanPhyto PharmacologyAnonymous100% (1)
- Vertigo DavidsonDokumen13 halamanVertigo DavidsonifahInayahBelum ada peringkat
- Panoramic Radiography 11Dokumen47 halamanPanoramic Radiography 11empormeniBelum ada peringkat