Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Polio, HPV, JeDokumen8 halamanPolio, HPV, JeTan Hing LeeBelum ada peringkat
- 2 - CNS QDokumen4 halaman2 - CNS QTan Hing LeeBelum ada peringkat
- Symptoms of PolyneuropathiesDokumen5 halamanSymptoms of PolyneuropathiesTan Hing LeeBelum ada peringkat
- Sigmoid Volvulus: Vertical Incision) (Suspected To Be Acute and Not ChronicDokumen3 halamanSigmoid Volvulus: Vertical Incision) (Suspected To Be Acute and Not ChronicTan Hing LeeBelum ada peringkat
- Causes: - Eg: Wrist Fracture, Swelling and Inflammation of Rheumatoid ArthritisDokumen1 halamanCauses: - Eg: Wrist Fracture, Swelling and Inflammation of Rheumatoid ArthritisTan Hing LeeBelum ada peringkat
- Causes: - Eg: Wrist Fracture, Swelling and Inflammation of Rheumatoid ArthritisDokumen1 halamanCauses: - Eg: Wrist Fracture, Swelling and Inflammation of Rheumatoid ArthritisTan Hing LeeBelum ada peringkat
- Postoperative MX LO 5 6Dokumen18 halamanPostoperative MX LO 5 6Tan Hing LeeBelum ada peringkat
- SeminarDokumen13 halamanSeminarTan Hing LeeBelum ada peringkat
- Malignant Sebaceous CA and LiposarcomaDokumen8 halamanMalignant Sebaceous CA and LiposarcomaTan Hing LeeBelum ada peringkat
- Causes: - Eg: Wrist Fracture, Swelling and Inflammation of Rheumatoid ArthritisDokumen1 halamanCauses: - Eg: Wrist Fracture, Swelling and Inflammation of Rheumatoid ArthritisTan Hing LeeBelum ada peringkat
- Obs and Gynar 4Dokumen3 halamanObs and Gynar 4Tan Hing LeeBelum ada peringkat
- Obs and Gynar 5Dokumen1 halamanObs and Gynar 5Tan Hing LeeBelum ada peringkat
- Causes: - Eg: Wrist Fracture, Swelling and Inflammation of Rheumatoid ArthritisDokumen1 halamanCauses: - Eg: Wrist Fracture, Swelling and Inflammation of Rheumatoid ArthritisTan Hing LeeBelum ada peringkat
- DysuriaDokumen4 halamanDysuriaTan Hing LeeBelum ada peringkat
- Medications For AntithromboticsDokumen4 halamanMedications For AntithromboticsTan Hing LeeBelum ada peringkat
- 9) Understand The Definition, Causes and Management of Hypoxia During AnaesthesiaDokumen7 halaman9) Understand The Definition, Causes and Management of Hypoxia During AnaesthesiaTan Hing LeeBelum ada peringkat
- Define The Local Anaesthetic DrugDokumen4 halamanDefine The Local Anaesthetic DrugTan Hing LeeBelum ada peringkat
- Anorectal Abscess BDokumen5 halamanAnorectal Abscess BTan Hing LeeBelum ada peringkat
- NutritionDokumen32 halamanNutritionTan Hing LeeBelum ada peringkat
- History Taking - Physical Examination - Lab Test: Investigate Cause of FeverDokumen6 halamanHistory Taking - Physical Examination - Lab Test: Investigate Cause of FeverTan Hing LeeBelum ada peringkat
- IsofluraneDokumen6 halamanIsofluraneTan Hing LeeBelum ada peringkat
- Postoperative MX LO 5 6Dokumen18 halamanPostoperative MX LO 5 6Tan Hing LeeBelum ada peringkat
- Davidson's McqsDokumen145 halamanDavidson's McqsSekhons Akademy100% (3)
- MCQ - Pharmacology LippincottDokumen48 halamanMCQ - Pharmacology Lippincottamwritea82% (22)
- 05 02 Rabbit Nerve ImpulseDokumen10 halaman05 02 Rabbit Nerve ImpulseTan Hing LeeBelum ada peringkat
- ETC, Oxidation Complexes and CofactorsDokumen30 halamanETC, Oxidation Complexes and CofactorsTan Hing LeeBelum ada peringkat
- TBL 1 Fever Q1 and Q2Dokumen5 halamanTBL 1 Fever Q1 and Q2Tan Hing LeeBelum ada peringkat
- Purpose of Sputum and Blood SampleDokumen2 halamanPurpose of Sputum and Blood SampleTan Hing LeeBelum ada peringkat
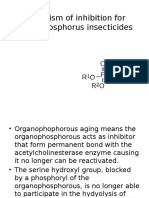
- Mechanism of Inhibition For Organophosphorus InsecticidesDokumen3 halamanMechanism of Inhibition For Organophosphorus InsecticidesTan Hing LeeBelum ada peringkat
- AnsLab Cell Injury InflammationDokumen26 halamanAnsLab Cell Injury InflammationTan Hing LeeBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Shy Doc Gave Good Face: Case StudyDokumen11 halamanShy Doc Gave Good Face: Case StudyIkkoBelum ada peringkat
- EC Certificate - Production Quality Assurance EC Certificate - Production Quality AssuranceDokumen6 halamanEC Certificate - Production Quality Assurance EC Certificate - Production Quality AssuranceEngr Hamid AliBelum ada peringkat
- Municipality of Buenavista, Bohol, Philippines - A Situational Analysis, IncompleteDokumen25 halamanMunicipality of Buenavista, Bohol, Philippines - A Situational Analysis, IncompleteMark Johnuel Duavis0% (1)
- LidocaineDokumen4 halamanLidocaineAhmad Fauzi100% (1)
- UntitledDokumen624 halamanUntitledjungleBelum ada peringkat
- Basics of Stem Cell TransplantDokumen46 halamanBasics of Stem Cell TransplantNarendra Bhattarai100% (5)
- Assignment 3Dokumen6 halamanAssignment 3ticticBelum ada peringkat
- Active and Passive Euthanasia Thesis StatementDokumen7 halamanActive and Passive Euthanasia Thesis StatementDoMyPaperForMeSingapore100% (2)
- Waksman 2018Dokumen7 halamanWaksman 2018harry pribadiBelum ada peringkat
- CME PRETERM LABOR, PROM, PPROM FDokumen39 halamanCME PRETERM LABOR, PROM, PPROM FRatna Setia WatiBelum ada peringkat
- Clinical Research As A CarreerDokumen37 halamanClinical Research As A Carreerrahil khanBelum ada peringkat
- Annexure To Health Sector Financing by Centre and States/Uts in India (2013-14 To 2015-16)Dokumen239 halamanAnnexure To Health Sector Financing by Centre and States/Uts in India (2013-14 To 2015-16)umeshBelum ada peringkat
- Muimar Sales PageDokumen3 halamanMuimar Sales PagePre Boy Ent.Belum ada peringkat
- SPC 124433Dokumen5 halamanSPC 124433abdelaziz_ismail685662Belum ada peringkat
- Health Hazards of Chemicals Commonly Used On Military BasesDokumen35 halamanHealth Hazards of Chemicals Commonly Used On Military Basesmale nurseBelum ada peringkat
- Oral Lymphoma PDFDokumen11 halamanOral Lymphoma PDFIcha Aisya AisyaBelum ada peringkat
- Bawasig Pediatric ExamDokumen20 halamanBawasig Pediatric Examخلدون سليمBelum ada peringkat
- Nimotuzumab A Novel anti-EGFR Monoclonal PDFDokumen8 halamanNimotuzumab A Novel anti-EGFR Monoclonal PDFAkbar SuuryoBelum ada peringkat
- Diabetic NeuropathyDokumen31 halamanDiabetic NeuropathyDEWI RIZKI AGUSTINABelum ada peringkat
- MS Soapie #1Dokumen2 halamanMS Soapie #1Fatima KateBelum ada peringkat
- Radiology and HoneyCombDokumen12 halamanRadiology and HoneyCombmuhhasanalbolkiah saidBelum ada peringkat
- PTCADokumen51 halamanPTCAJasmin Jacob100% (1)
- 2018 HIV GuidelinesDokumen125 halaman2018 HIV GuidelinesAndrew KaumbaBelum ada peringkat
- Covid-19 Pandamic by PriyanshDokumen5 halamanCovid-19 Pandamic by PriyanshShri ram PujariBelum ada peringkat
- Ethical and Legal Issues in Reproductive HealthDokumen4 halamanEthical and Legal Issues in Reproductive HealthBianca_P0pBelum ada peringkat
- Attachment 5 - Crew Health Declaration - 2015-09 - Ver0 (5) 2Dokumen1 halamanAttachment 5 - Crew Health Declaration - 2015-09 - Ver0 (5) 2Julessio SihombingBelum ada peringkat
- Foot DropDokumen2 halamanFoot DropSaravanan SridharanBelum ada peringkat
- Felix Widal TestDokumen9 halamanFelix Widal TestGaluhAlvianaBelum ada peringkat
- Admission To NICU CA4068v3Dokumen12 halamanAdmission To NICU CA4068v3Hana ChristyantiBelum ada peringkat