Anda mungkin juga menyukai
- RenalDokumen8 halamanRenalLoislane RullBelum ada peringkat
- 1.4 Virtual Patient - Elizabeth Harding: Describe The Structure of The NephronDokumen7 halaman1.4 Virtual Patient - Elizabeth Harding: Describe The Structure of The NephronAbdullah RajaBelum ada peringkat
- Renal (Urinary) SystemDokumen51 halamanRenal (Urinary) SystempolandekaBelum ada peringkat
- Form 5 Biology: Chapter 3 .3 HomeostasisDokumen12 halamanForm 5 Biology: Chapter 3 .3 HomeostasisZifan NafriBelum ada peringkat
- The Urinary System: Pembentukan Urin Dan Peran Ginjal Dalam Keseimbangan Cairan TubuhDokumen64 halamanThe Urinary System: Pembentukan Urin Dan Peran Ginjal Dalam Keseimbangan Cairan TubuhYunan Syahban MaskatBelum ada peringkat
- Functions of The Urinary System Anatomy of The Kidney Urine FormationDokumen71 halamanFunctions of The Urinary System Anatomy of The Kidney Urine FormationmaninagaBelum ada peringkat
- Renal Physiology NotesDokumen6 halamanRenal Physiology Notescipa920% (1)
- Chapter 25Dokumen55 halamanChapter 25Chuy Cantu RdzBelum ada peringkat
- Biology 7C 1Dokumen4 halamanBiology 7C 1Abdullayev KamranBelum ada peringkat
- Anaesthesia in Renal Failure: Nadia Van Heerden Kimberley Hospital Complex 30 January 2015Dokumen56 halamanAnaesthesia in Renal Failure: Nadia Van Heerden Kimberley Hospital Complex 30 January 2015Khaeril IrfanBelum ada peringkat
- Renal FunctionDokumen6 halamanRenal FunctionRia AlcantaraBelum ada peringkat
- Urine Formation: Joanna I. Alafag Adv. Animal Physiology Feb. 13, 2020Dokumen64 halamanUrine Formation: Joanna I. Alafag Adv. Animal Physiology Feb. 13, 2020Tyron Cadiz LopezBelum ada peringkat
- A Share WATER & ELECTROLYTE BALANCEDokumen14 halamanA Share WATER & ELECTROLYTE BALANCENaaz creates creativeBelum ada peringkat
- Chapter 16 ReviewDokumen21 halamanChapter 16 Reviewjenn1722Belum ada peringkat
- Urinalysis and Body FluidsDokumen54 halamanUrinalysis and Body FluidsabdishakurBelum ada peringkat
- Urine Formation and ExcretionDokumen12 halamanUrine Formation and ExcretionNilesh SawantBelum ada peringkat
- Concept Map UrinaryDokumen3 halamanConcept Map UrinarySharan Kaur90% (10)
- Physiology of Urine Formation: Submitted To - Mr. Pankaj Gupta Sir Department of ZoologyDokumen15 halamanPhysiology of Urine Formation: Submitted To - Mr. Pankaj Gupta Sir Department of ZoologyRajeshwer duttBelum ada peringkat
- Filtrasi GlomerulusDokumen41 halamanFiltrasi GlomerulusFaishalBelum ada peringkat
- Renal Physiology: Done byDokumen28 halamanRenal Physiology: Done byJanine Marie Kathleen Uy-CuanangBelum ada peringkat
- Renal SystemDokumen38 halamanRenal SystemSampat KumarBelum ada peringkat
- 17 Osmoregulation IIDokumen54 halaman17 Osmoregulation IIJerilee SoCute WattsBelum ada peringkat
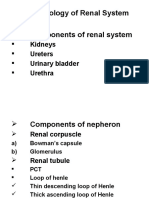
- Pharmacology of Renal System Components of Renal System: Kidneys Ureters Urinary Bladder UrethraDokumen30 halamanPharmacology of Renal System Components of Renal System: Kidneys Ureters Urinary Bladder UrethraMirza HassanBelum ada peringkat
- How Do The Kidneys Control Things?: Why Do We Need To Maintain It?Dokumen14 halamanHow Do The Kidneys Control Things?: Why Do We Need To Maintain It?api-246259817Belum ada peringkat
- PhysiologyDokumen85 halamanPhysiologyDyah WahliaBelum ada peringkat
- Practice Questions For Function of The Urinary System-AnswersDokumen16 halamanPractice Questions For Function of The Urinary System-AnswersDebra Gan100% (1)
- XQ WFHKLJW WWHAfu 0 DGWFDokumen10 halamanXQ WFHKLJW WWHAfu 0 DGWFGiridharan & Balaji RNBelum ada peringkat
- KidneyDokumen8 halamanKidneyRaj JadhavBelum ada peringkat
- The Urinary System: Dr. Sri Lestari Sulistyo RiniDokumen42 halamanThe Urinary System: Dr. Sri Lestari Sulistyo Riniummu husnaBelum ada peringkat
- Excretory SystemDokumen37 halamanExcretory SystemPatrick DeeBelum ada peringkat
- CH 26 UrinaryDokumen63 halamanCH 26 Urinaryaijaz1inBelum ada peringkat
- Urinary System: G G R O U P 4 - B S N 1 - 5Dokumen59 halamanUrinary System: G G R O U P 4 - B S N 1 - 5Love Jovellanos ÜBelum ada peringkat
- 10 Renal Physiology FKDokumen139 halaman10 Renal Physiology FKStephen PramatyaBelum ada peringkat
- HWF 2961 58522 HomeostasisandExcretionRevisionXOLBiologyDokumen14 halamanHWF 2961 58522 HomeostasisandExcretionRevisionXOLBiologybasima jawaidBelum ada peringkat
- ExcretionDokumen17 halamanExcretionsmbdy tbhhhBelum ada peringkat
- D - Renal PhysiologyDokumen26 halamanD - Renal PhysiologyMohamad Zekry ZuhairyBelum ada peringkat
- Urinary System: by Eka BebasariDokumen47 halamanUrinary System: by Eka BebasariMuhammad Reza SaputraBelum ada peringkat
- Drugs Affecting Urinary SystemDokumen19 halamanDrugs Affecting Urinary SystemdionyessBelum ada peringkat
- FLG 332 Renal Physiology - 1 (2019)Dokumen58 halamanFLG 332 Renal Physiology - 1 (2019)Huzaifa KhanBelum ada peringkat
- K10 Kuliah NefrourologiDokumen170 halamanK10 Kuliah NefrourologimarinanananaBelum ada peringkat
- Excreatory System1Dokumen123 halamanExcreatory System1mazna khalilBelum ada peringkat
- Hormonal RegulationDokumen12 halamanHormonal RegulationPratiksha JhareeBelum ada peringkat
- Mechanism and Regulation of Urine Formation Part 1Dokumen5 halamanMechanism and Regulation of Urine Formation Part 1Zi .aBelum ada peringkat
- Gin Jal Warn A Animal 2010Dokumen65 halamanGin Jal Warn A Animal 2010ghe_vrayBelum ada peringkat
- Excretion ExcretionDokumen7 halamanExcretion ExcretionWaleed Bin KhalidBelum ada peringkat
- UrinaryDokumen87 halamanUrinaryJohn Paolo Dalida SalazarBelum ada peringkat
- General Principles of Tubular ReabsorptionDokumen54 halamanGeneral Principles of Tubular ReabsorptionRalph JacintoBelum ada peringkat
- STUDY NOTES-The Urinary SystemDokumen3 halamanSTUDY NOTES-The Urinary Systempeterneil75% (4)
- Excretory SystemDokumen47 halamanExcretory Systemalice mamaBelum ada peringkat
- Renal PhysiologyDokumen7 halamanRenal PhysiologyambiliBelum ada peringkat
- Kuliah 1 Proses Pembentukan UrineDokumen30 halamanKuliah 1 Proses Pembentukan UrineImpi SusantiBelum ada peringkat
- Topic 6 - Excretory System 2021Dokumen49 halamanTopic 6 - Excretory System 2021Ralph Rezin MooreBelum ada peringkat
- Medical Surgical Nursing Lecture Support of Renal Function and MODS 11152022 ShortDokumen16 halamanMedical Surgical Nursing Lecture Support of Renal Function and MODS 11152022 Shortje-ann catedralBelum ada peringkat
- The Human Excretory SystemDokumen7 halamanThe Human Excretory Systemdonnah_veraBelum ada peringkat
- Chapter-19 Excretory Products and Their Elimnation: Forms of Nitrogen ExcretionsDokumen8 halamanChapter-19 Excretory Products and Their Elimnation: Forms of Nitrogen Excretionsmaryak3050Belum ada peringkat
- Sken D Blok 20 Kel 2 '17Dokumen18 halamanSken D Blok 20 Kel 2 '17dewi fortuna agustiaBelum ada peringkat
- Renal Perfusion and Filtration: Alan Stephenson BBSG 503 - Systems BiologyDokumen38 halamanRenal Perfusion and Filtration: Alan Stephenson BBSG 503 - Systems BiologyAfsaneh JavanmardBelum ada peringkat
- Urinary Tract PhysiologykulDokumen72 halamanUrinary Tract PhysiologykulAya KamajayaBelum ada peringkat
- Ascites, A Simple Guide To The Condition, Treatment And Related ConditionsDari EverandAscites, A Simple Guide To The Condition, Treatment And Related ConditionsBelum ada peringkat
- Perfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationDari EverandPerfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationPenilaian: 5 dari 5 bintang5/5 (2)