Anda mungkin juga menyukai
- Bone Healing and Non UnionsDokumen50 halamanBone Healing and Non UnionsFelicia BockBelum ada peringkat
- Practice Of Osteopathy - Its Practical Application To The Various Diseases Of The Human BodyDari EverandPractice Of Osteopathy - Its Practical Application To The Various Diseases Of The Human BodyPenilaian: 5 dari 5 bintang5/5 (1)
- Orthopaedics Diagnosis & Therapy: Dr. Su Djie To Rante, M.Biomed, SP - OTDokumen75 halamanOrthopaedics Diagnosis & Therapy: Dr. Su Djie To Rante, M.Biomed, SP - OTDiana MarcusBelum ada peringkat
- Principles Fracture ManagementDokumen88 halamanPrinciples Fracture ManagementYauffa Hanna Elt MisykahBelum ada peringkat
- Basics of FractureDokumen12 halamanBasics of Fracturecimahmudraju100% (2)
- Osteomyelitis: Pathophysiology & Treatment Decisions: Clifford B. Jones, MDDokumen63 halamanOsteomyelitis: Pathophysiology & Treatment Decisions: Clifford B. Jones, MDRose Ann Del MundoBelum ada peringkat
- New Microsoft Power Point PresentationDokumen20 halamanNew Microsoft Power Point PresentationAkram KhatriBelum ada peringkat
- Non Union 110219161100 Phpapp02Dokumen41 halamanNon Union 110219161100 Phpapp02Deep Katyan DeepBelum ada peringkat
- Traumatology Exam Questions AnswersDokumen92 halamanTraumatology Exam Questions AnswersElo GonçalvesBelum ada peringkat
- Final - Open Fracture Classification & Limb Salvage in TraumaDokumen13 halamanFinal - Open Fracture Classification & Limb Salvage in TraumaGraceBelum ada peringkat
- SURGICAL TALK FinalpptDokumen30 halamanSURGICAL TALK FinalpptRazeen RiyasatBelum ada peringkat
- Poorly Nourished Elderly Obese Impaired Immune System Chronic Illness Receiving Long Term Corticosteroid TherapyDokumen182 halamanPoorly Nourished Elderly Obese Impaired Immune System Chronic Illness Receiving Long Term Corticosteroid TherapyjhaninahBelum ada peringkat
- Degenerative Sport (Autosaved)Dokumen71 halamanDegenerative Sport (Autosaved)Elisabeth Permatasari SidabutarBelum ada peringkat
- IT 1 Introduction Blok 22 - PRMDokumen18 halamanIT 1 Introduction Blok 22 - PRMApriyani Supia DewiBelum ada peringkat
- Spondylosis, Degeneration of Intervertebral Disc Diagnosis/Condition: ICD-9 CodesDokumen4 halamanSpondylosis, Degeneration of Intervertebral Disc Diagnosis/Condition: ICD-9 CodesAloysius DicodemusBelum ada peringkat
- Orthopedic Essentials in Emergency MedicineDokumen35 halamanOrthopedic Essentials in Emergency MedicineMohd Tarmizi100% (1)
- NEW INJECTION PALSY PRTDokumen25 halamanNEW INJECTION PALSY PRTChidube UkachukwuBelum ada peringkat
- Fracture: Edfran Jed A. Serino MSN 303Dokumen34 halamanFracture: Edfran Jed A. Serino MSN 303Edfran Jed SerinoBelum ada peringkat
- Introduction To The Musculoskeletal SystemDokumen39 halamanIntroduction To The Musculoskeletal SystemdesyBelum ada peringkat
- Lower Back Pain: DR Robert Ramcharan MBBS, Frcsed, DM (Neurosurgery) NeurosurgeonDokumen69 halamanLower Back Pain: DR Robert Ramcharan MBBS, Frcsed, DM (Neurosurgery) NeurosurgeonShimmering MoonBelum ada peringkat
- Ortho EssentialDokumen39 halamanOrtho EssentialaninuninBelum ada peringkat
- Fracture ClassificationDokumen50 halamanFracture ClassificationsrhubanbabuBelum ada peringkat
- Update A1 OsceDokumen120 halamanUpdate A1 OsceIndra SetyaBelum ada peringkat
- 1-22 Osteoporosis & Hip PainDokumen79 halaman1-22 Osteoporosis & Hip PaintarikeopsBelum ada peringkat
- Handout Lat Elbow Pain PDFDokumen47 halamanHandout Lat Elbow Pain PDFgemichan26Belum ada peringkat
- Osteoarthritis: A. Pusey Murray (MRS)Dokumen25 halamanOsteoarthritis: A. Pusey Murray (MRS)okaciaBelum ada peringkat
- Pengayaan Koass Ortho - Update 5 VersionDokumen122 halamanPengayaan Koass Ortho - Update 5 Versionanon_967171484Belum ada peringkat
- Osteopathic Manipulation Techniques (OMT) .: Becoming Familiar With Basic PrinciplesDokumen54 halamanOsteopathic Manipulation Techniques (OMT) .: Becoming Familiar With Basic PrinciplesRoberto CarvalhoBelum ada peringkat
- Fracture Healing: Tony Olasinde Dept of Surgery, Faculty of Clinical Medicine and Dentistry KIU (Western Campus) IshakaDokumen22 halamanFracture Healing: Tony Olasinde Dept of Surgery, Faculty of Clinical Medicine and Dentistry KIU (Western Campus) IshakaOlasinde AnthonyBelum ada peringkat
- Osteoarthritis of The Knee HKDokumen31 halamanOsteoarthritis of The Knee HKFira Wahidah FirdausBelum ada peringkat
- Osteomyelitis: Staphylococcus Aureus Is The Mosy Common Infecting Microorganisms FollowingDokumen8 halamanOsteomyelitis: Staphylococcus Aureus Is The Mosy Common Infecting Microorganisms FollowingSharah LondonioBelum ada peringkat
- Osteoarthritis: Prepared by Dr/Mohammed AlshehariDokumen17 halamanOsteoarthritis: Prepared by Dr/Mohammed AlsheharimosaBelum ada peringkat
- Compression FractureDokumen4 halamanCompression FracturepuchioBelum ada peringkat
- Lateral and Medial EpicondylitisDokumen40 halamanLateral and Medial EpicondylitisVijay PradeepBelum ada peringkat
- OsteoarthritisDokumen40 halamanOsteoarthritiskylieverBelum ada peringkat
- Lect 6Dokumen37 halamanLect 6eslambasuony98Belum ada peringkat
- 13 - Musculoskeletal System AssessmentDokumen53 halaman13 - Musculoskeletal System Assessmente.mb275Belum ada peringkat
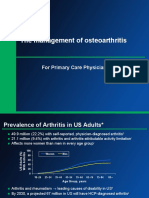
- The Management of Osteoarthritis: For Primary Care PhysicianDokumen46 halamanThe Management of Osteoarthritis: For Primary Care PhysicianMaida FitrianiBelum ada peringkat
- OU Shoulder and Elbow OITE Review: September 23, 2015 Betsy M. Nolan MDDokumen159 halamanOU Shoulder and Elbow OITE Review: September 23, 2015 Betsy M. Nolan MDJayBelum ada peringkat
- Osteoarthritis 191016103144Dokumen49 halamanOsteoarthritis 191016103144dr.abouzaid098Belum ada peringkat
- GRON3112 Basic Care in Gerontology L.8 Pain Management For Older Adults Week 10 2022.11.08 PDFDokumen31 halamanGRON3112 Basic Care in Gerontology L.8 Pain Management For Older Adults Week 10 2022.11.08 PDF2K FaustusBelum ada peringkat
- Pembahasan TTG FrakturDokumen48 halamanPembahasan TTG FrakturErik Ad'perdianBelum ada peringkat
- Askep Pada Pasien Dengan Kerusakan Multi SistemDokumen76 halamanAskep Pada Pasien Dengan Kerusakan Multi SistemmeldaiskaBelum ada peringkat
- New Introduction To Ortho 1 Jan 20016Dokumen67 halamanNew Introduction To Ortho 1 Jan 20016BIOLOGY BY ISMAIL ANSARIBelum ada peringkat
- Osteomyelitis - Kaye WilkinsDokumen50 halamanOsteomyelitis - Kaye WilkinsWindy MentariBelum ada peringkat
- Low Back Pain WMDokumen19 halamanLow Back Pain WMvandhani79Belum ada peringkat
- Lecture 7 Femoral Diapisis and Distal FDokumen16 halamanLecture 7 Femoral Diapisis and Distal FQueen SofiaBelum ada peringkat
- אוסטיאומיאליטיס ושברים פתוחיםDokumen68 halamanאוסטיאומיאליטיס ושברים פתוחיםHussein SamhatBelum ada peringkat
- G06 FX Classification JTG Rev 2-3-10Dokumen50 halamanG06 FX Classification JTG Rev 2-3-10KURBULDKBelum ada peringkat
- Delayed & Non UnionDokumen23 halamanDelayed & Non UniondiozBelum ada peringkat
- Osteoid OsteomaDokumen24 halamanOsteoid Osteomadrqazi777Belum ada peringkat
- Fracture Healing: Presenter: DR Mugi Ortho ResidentDokumen32 halamanFracture Healing: Presenter: DR Mugi Ortho ResidentPhoenix MerchantsBelum ada peringkat
- Anatomy 3Dokumen52 halamanAnatomy 3Balsam TeineBelum ada peringkat
- Fractures - Diagnosis and ManagementDokumen28 halamanFractures - Diagnosis and ManagementdrthanallaBelum ada peringkat
- Musculoskeletal SystemDokumen44 halamanMusculoskeletal Systemayesharajput5110Belum ada peringkat
- Section 1: General OrthopaedicsDokumen25 halamanSection 1: General OrthopaedicsAditio PranandaBelum ada peringkat
- OADokumen27 halamanOADarkKnighthere100% (1)
- MS 36Dokumen7 halamanMS 36jefrocBelum ada peringkat
- ANYLYZERDokumen1 halamanANYLYZERDeep Katyan DeepBelum ada peringkat
- ANYLYZERDokumen1 halamanANYLYZERDeep Katyan DeepBelum ada peringkat
- Femoral Neck Fractures: Steven A. Olson, MDDokumen54 halamanFemoral Neck Fractures: Steven A. Olson, MDCha ParaynoBelum ada peringkat
- Anatomy and ImagingDokumen19 halamanAnatomy and ImagingDeep Katyan DeepBelum ada peringkat
- Locked Plating: Sean E. Nork, MD James P. Stannard, MD and Philip J. Kregor, MDDokumen119 halamanLocked Plating: Sean E. Nork, MD James P. Stannard, MD and Philip J. Kregor, MDDeep Katyan DeepBelum ada peringkat
- H PyloriDokumen1 halamanH PyloriDeep Katyan DeepBelum ada peringkat
- Non Union 110219161100 Phpapp02Dokumen41 halamanNon Union 110219161100 Phpapp02Deep Katyan DeepBelum ada peringkat
- G05 - Ards - Fes - DVT - PeDokumen65 halamanG05 - Ards - Fes - DVT - PeDeep Katyan DeepBelum ada peringkat
- Orthobiologics: J. Tracy Watson, MDDokumen130 halamanOrthobiologics: J. Tracy Watson, MDDeep Katyan DeepBelum ada peringkat
- G21 OsteomyelitisDokumen98 halamanG21 OsteomyelitisDeep Katyan DeepBelum ada peringkat
- L03 Intertrochanteric FXDokumen102 halamanL03 Intertrochanteric FXDeep Katyan Deep100% (1)
- Hip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDDokumen97 halamanHip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDLassie LazyBelum ada peringkat
- Femoral Shaft Fractures: Robert F. Ostrum, MDDokumen81 halamanFemoral Shaft Fractures: Robert F. Ostrum, MDDeep Katyan DeepBelum ada peringkat
- General INDEXDokumen1 halamanGeneral INDEXDeep Katyan DeepBelum ada peringkat
- G20 Nonunions With DefectsDokumen69 halamanG20 Nonunions With DefectsDeep Katyan DeepBelum ada peringkat
- INTRO PpsDokumen3 halamanINTRO PpsDeep Katyan DeepBelum ada peringkat
- Initial Assessment and Management of The Multiply Injured PatientDokumen48 halamanInitial Assessment and Management of The Multiply Injured PatientDeep Katyan DeepBelum ada peringkat
- G24 Fragility FracturesDokumen38 halamanG24 Fragility FracturesDeep Katyan DeepBelum ada peringkat
- General Principles in The Assessment and Treatment of NonunionsDokumen63 halamanGeneral Principles in The Assessment and Treatment of NonunionsDeep Katyan DeepBelum ada peringkat
- G06 Fracture ClassificationDokumen39 halamanG06 Fracture ClassificationWaNda GrBelum ada peringkat
- G19 NonunionsDokumen72 halamanG19 NonunionsDeep Katyan DeepBelum ada peringkat
- G17 Pathologic FxsDokumen56 halamanG17 Pathologic FxsDeep Katyan DeepBelum ada peringkat
- G22 Outcome ImpairmentDokumen37 halamanG22 Outcome ImpairmentDeep Katyan DeepBelum ada peringkat
- G15 Wound Tech Inj ExtremDokumen55 halamanG15 Wound Tech Inj ExtremDeep Katyan DeepBelum ada peringkat
- Bone Grafting and Bone Graft Substitutes: David Hak, MDDokumen57 halamanBone Grafting and Bone Graft Substitutes: David Hak, MDDeep Katyan DeepBelum ada peringkat
- G10 Internal Fix PrinciplesDokumen54 halamanG10 Internal Fix PrinciplesDeep Katyan DeepBelum ada peringkat
- Epidemiology, Diagnosis Prevention and Management of Osteoporotic FracturesDokumen69 halamanEpidemiology, Diagnosis Prevention and Management of Osteoporotic Fracturesnfacma100% (2)
- G13 Fxs W Soft Tissue InjDokumen60 halamanG13 Fxs W Soft Tissue InjDeep Katyan DeepBelum ada peringkat
- G14 GSW FxsDokumen52 halamanG14 GSW FxsDeep Katyan DeepBelum ada peringkat
- G11 Ex Fix PrinciplesDokumen66 halamanG11 Ex Fix PrinciplesDeep Katyan DeepBelum ada peringkat