Anda mungkin juga menyukai
- Viral Hepatitis and Blood Glucose ReportsDokumen5 halamanViral Hepatitis and Blood Glucose ReportsJunaid Ahmad100% (1)
- Practical Hemostasis and ThrombosisDari EverandPractical Hemostasis and ThrombosisNigel S. KeyBelum ada peringkat
- Biomechanic of MuscleDokumen45 halamanBiomechanic of MuscleRonak Patel100% (1)
- Biolab: Animal Tissues Lab Report Name, Date, Course and Section Required For Password: 1409Dokumen5 halamanBiolab: Animal Tissues Lab Report Name, Date, Course and Section Required For Password: 1409RosaBelum ada peringkat
- Disseminated Intravascular Coagulation - Background, Pathophysiology, EtiologyDokumen11 halamanDisseminated Intravascular Coagulation - Background, Pathophysiology, Etiologyevi100% (2)
- Hematology Pathology - 002) CBC - Approach To Polycythemia (Notes)Dokumen4 halamanHematology Pathology - 002) CBC - Approach To Polycythemia (Notes)Aro DanaBelum ada peringkat
- Disseminated Intravascular CoagulationDokumen37 halamanDisseminated Intravascular CoagulationAlfitoHarfahGiffaryBelum ada peringkat
- Dic - MNJDokumen36 halamanDic - MNJmaibejoseBelum ada peringkat
- Disseminated Intravascular Coagulation: Keith Lewis, MDDokumen37 halamanDisseminated Intravascular Coagulation: Keith Lewis, MDTimea DaniBelum ada peringkat
- Disseminated Intravascular Coagulation: Keith Lewis, MDDokumen29 halamanDisseminated Intravascular Coagulation: Keith Lewis, MDjyothinanduriBelum ada peringkat
- Coagulation DisordersDokumen26 halamanCoagulation DisordersLia pramita0% (1)
- Coagulation DisordersDokumen26 halamanCoagulation DisordersLia pramitaBelum ada peringkat
- Hemostasis, Clotting Disorder and AnticoagulantsDokumen87 halamanHemostasis, Clotting Disorder and AnticoagulantsSomit Jain100% (1)
- Approach To Bleeding Child: Moderator: Dr. Ayal (MD, Pediatrician) Presenters: Wubshet K. & Yihenew D. (C-I Students)Dokumen92 halamanApproach To Bleeding Child: Moderator: Dr. Ayal (MD, Pediatrician) Presenters: Wubshet K. & Yihenew D. (C-I Students)woldemariamBelum ada peringkat
- Bleeding DisorderDokumen56 halamanBleeding DisorderPriya Singh100% (1)
- AssignmentDokumen11 halamanAssignmentrehamoh1997Belum ada peringkat
- Bleeding and Coagulation Disorders: DR Nidhi Chaurasia JR-1 MDS PedodonticsDokumen66 halamanBleeding and Coagulation Disorders: DR Nidhi Chaurasia JR-1 MDS PedodonticsDrNidhi KrishnaBelum ada peringkat
- 25. Coagulation Disorders in PregnancyDokumen35 halaman25. Coagulation Disorders in PregnancyMuwanga faizoBelum ada peringkat
- DICDokumen60 halamanDICAbhineet SalveBelum ada peringkat
- Disseminated Intravascular Coagulopathy: D.I.C Specific Learning ObjectivesDokumen15 halamanDisseminated Intravascular Coagulopathy: D.I.C Specific Learning ObjectivesmartinBelum ada peringkat
- Pathology Bleeding DisordersDokumen67 halamanPathology Bleeding DisordersMarcelliaBelum ada peringkat
- Clinical Manifestations of DICDokumen25 halamanClinical Manifestations of DICAbdulaziz SassiBelum ada peringkat
- Coag Unit 6 Notes Coagdisorders Secondary F08Dokumen25 halamanCoag Unit 6 Notes Coagdisorders Secondary F08Nadir A IbrahimBelum ada peringkat
- Complex Process Terminates Blood Loss From The Intravascular SpaceDokumen25 halamanComplex Process Terminates Blood Loss From The Intravascular SpaceDewi YukinohanaBelum ada peringkat
- Hematologic Pathology p1-23Dokumen23 halamanHematologic Pathology p1-23zeroun24100% (2)
- Disorders Leading To ThrombosisDokumen27 halamanDisorders Leading To ThrombosisFearless AngelBelum ada peringkat
- Bleeding TimeDokumen47 halamanBleeding Timechickenbacon34Belum ada peringkat
- Coagulation Disorders in ICUDokumen72 halamanCoagulation Disorders in ICUMadhusudan H C Gowda100% (1)
- Coagulation Disorders in Obstetrics MD5Dokumen51 halamanCoagulation Disorders in Obstetrics MD5gloriashirima8Belum ada peringkat
- Hema 2 5th Ed SummaryDokumen9 halamanHema 2 5th Ed Summarymonzon.mika1801Belum ada peringkat
- Bleeding Time, Clotting Time PT and PTT2Dokumen41 halamanBleeding Time, Clotting Time PT and PTT2Qurrataini Ibanez100% (1)
- Coagulacion Intravascular Diseminada: Hospital General Agustin O' HoranDokumen41 halamanCoagulacion Intravascular Diseminada: Hospital General Agustin O' Horanefrain_arceBelum ada peringkat
- Disseminated Intravascular CoagualationDokumen47 halamanDisseminated Intravascular CoagualationIshaBrijeshSharmaBelum ada peringkat
- Management of Acquired Coagulation Disorders in Emergency and Intensive-Care MedicineDokumen12 halamanManagement of Acquired Coagulation Disorders in Emergency and Intensive-Care Medicineshinichi kudoBelum ada peringkat
- Lecture 5Dokumen48 halamanLecture 5Ahed ShaerBelum ada peringkat
- Disseminated Intravascular Coagulation: Quratulain Mughal Batch Iv Iirs, Iukc Doctor PF Physical TherapyDokumen24 halamanDisseminated Intravascular Coagulation: Quratulain Mughal Batch Iv Iirs, Iukc Doctor PF Physical TherapyMuhammadBelum ada peringkat
- Coagulation: Bleeding TimeDokumen6 halamanCoagulation: Bleeding TimeimperiouxxBelum ada peringkat
- Understanding Hemostasis and ThrombosisDokumen77 halamanUnderstanding Hemostasis and ThrombosisFachdepy Maulana NgangiBelum ada peringkat
- G G G G G GDokumen16 halamanG G G G G Gpreeti19987Belum ada peringkat
- Platelet Storage Pool Disorders PDFDokumen4 halamanPlatelet Storage Pool Disorders PDFMano CempakaBelum ada peringkat
- Key Terms: Chapter 19: Coagulation DisordersDokumen16 halamanKey Terms: Chapter 19: Coagulation DisordersDarryl Betts100% (1)
- Disseminated Intravascular Coagulopathy Disseminated Intravascular Coagulation (DIC) Is A PathologicalDokumen6 halamanDisseminated Intravascular Coagulopathy Disseminated Intravascular Coagulation (DIC) Is A PathologicalValarmathiBelum ada peringkat
- The Clotting Cascade and DIC: Karim Rafaat, MDDokumen33 halamanThe Clotting Cascade and DIC: Karim Rafaat, MDKathleenDawalBelum ada peringkat
- Why Does My Patient Have Thrombocytopenia PDFDokumen22 halamanWhy Does My Patient Have Thrombocytopenia PDFElena Villarreal100% (1)
- Disseminated Intravascular Coagulation: Treat The Cause, Not The Lab ValuesDokumen9 halamanDisseminated Intravascular Coagulation: Treat The Cause, Not The Lab Valuesboris_beroizaBelum ada peringkat
- Week 5: Trigger 3 Theme of The Week: Haemostasis: Full Blood CountDokumen30 halamanWeek 5: Trigger 3 Theme of The Week: Haemostasis: Full Blood CountFrances Lau Yee ChinBelum ada peringkat
- Disorder of PlateletsDokumen27 halamanDisorder of PlateletsRoby KieranBelum ada peringkat
- Fourth Stage HemostasisDokumen9 halamanFourth Stage HemostasisAli MOBelum ada peringkat
- Bleeding in Children SmsDokumen65 halamanBleeding in Children SmsAnastasiafynnBelum ada peringkat
- ThrombocytopeniaDokumen9 halamanThrombocytopeniaamjad_muslehBelum ada peringkat
- Treatment of Hemostasis DisordersDokumen17 halamanTreatment of Hemostasis DisordersDiana HyltonBelum ada peringkat
- Cogulation Profile: Bleeding Time, Clotting Time, PT, and PTTDokumen49 halamanCogulation Profile: Bleeding Time, Clotting Time, PT, and PTTDorin PathakBelum ada peringkat
- Hemostasis in the Surgical PatientDokumen39 halamanHemostasis in the Surgical Patientninjahattori1Belum ada peringkat
- Hema QuizletDokumen15 halamanHema QuizletFaith Theresa OroscoBelum ada peringkat
- Disorders of HaemostasisDokumen4 halamanDisorders of HaemostasisdeblackaBelum ada peringkat
- Hemostatic Complications of Solid OrganDokumen18 halamanHemostatic Complications of Solid OrganWael AlkhiaryBelum ada peringkat
- Surgery FinalDokumen6 halamanSurgery FinalMaebritt TibubosBelum ada peringkat
- 1 s2.0 S0899588513000701 Main PDFDokumen8 halaman1 s2.0 S0899588513000701 Main PDFRicki HanBelum ada peringkat
- Literature AbdoDokumen20 halamanLiterature AbdothestaffforpediatricptBelum ada peringkat
- Learning Outcome 1 Learning Outcome 2: (Osborn) Chapter 63 Learning Outcomes (Number and Title)Dokumen19 halamanLearning Outcome 1 Learning Outcome 2: (Osborn) Chapter 63 Learning Outcomes (Number and Title)KittiesBelum ada peringkat
- Trombocytopenia Uniba 16-1-13Dokumen32 halamanTrombocytopenia Uniba 16-1-13Dwiki Surya PrayogaBelum ada peringkat
- DIC Pregnancy 2009 PDFDokumen2 halamanDIC Pregnancy 2009 PDFGebbyBelum ada peringkat
- Disseminated Intravascular Coagulation: Dr. Rudy Afriant, Sppd-KhomDokumen22 halamanDisseminated Intravascular Coagulation: Dr. Rudy Afriant, Sppd-Khomsonnya morisaBelum ada peringkat
- 13 LansiaDokumen67 halaman13 LansiaPutri UtamiBelum ada peringkat
- 12-Kesehatan AnakDokumen88 halaman12-Kesehatan AnakPutri UtamiBelum ada peringkat
- 8-Tempat YankesDokumen44 halaman8-Tempat YankesPutri UtamiBelum ada peringkat
- 6-Sampah Dan PekaranganDokumen44 halaman6-Sampah Dan PekaranganPutri UtamiBelum ada peringkat
- 11 Asi EksklusifDokumen23 halaman11 Asi EksklusifPutri UtamiBelum ada peringkat
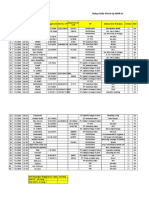
- Daily Check Up Report at Balongan LPG DepotDokumen3 halamanDaily Check Up Report at Balongan LPG DepotPutri UtamiBelum ada peringkat
- 9-Keluarga BerencanaDokumen67 halaman9-Keluarga BerencanaPutri UtamiBelum ada peringkat
- 4 SanitasiDokumen44 halaman4 SanitasiPutri UtamiBelum ada peringkat
- Rekap Daily Check Up MOR IIIDokumen5 halamanRekap Daily Check Up MOR IIIPutri UtamiBelum ada peringkat
- 15-08-2018Dokumen7 halaman15-08-2018Putri UtamiBelum ada peringkat
- Penatalaksanaan StrokeDokumen30 halamanPenatalaksanaan StrokePutri Utami100% (1)
- Laporan DCU MOR III LPG Balongan Juli 2019Dokumen116 halamanLaporan DCU MOR III LPG Balongan Juli 2019Putri UtamiBelum ada peringkat
- Nccu. Lampiran Lembar ObservasiDokumen1 halamanNccu. Lampiran Lembar ObservasiPutri UtamiBelum ada peringkat
- Daftar PustakaDokumen2 halamanDaftar PustakaaangedeBelum ada peringkat
- B Blab 6 Crossmatch SP 05Dokumen14 halamanB Blab 6 Crossmatch SP 05Rutchelle Joyce PugoyBelum ada peringkat
- المحاضرة الثالثةDokumen6 halamanالمحاضرة الثالثةNajwa AbdualgaderBelum ada peringkat
- SC ProjectDokumen5 halamanSC ProjectZijieBelum ada peringkat
- Thalassemia Case in 4-Year Old BoyDokumen30 halamanThalassemia Case in 4-Year Old BoyYama Sirly PutriBelum ada peringkat
- Effect of Blood Viscosity on Flow RateDokumen4 halamanEffect of Blood Viscosity on Flow RateKai ChenBelum ada peringkat
- Withdraw Blood SamplesDokumen18 halamanWithdraw Blood SamplesKomal fatimaBelum ada peringkat
- WBC CountingDokumen4 halamanWBC CountingMarx AsuncionBelum ada peringkat
- Complete Blood Count-2023-08-29t00 - 00 - 00Dokumen2 halamanComplete Blood Count-2023-08-29t00 - 00 - 00Michamiel SerratoBelum ada peringkat
- Transport System 2Dokumen4 halamanTransport System 2Ashley ArnoldBelum ada peringkat
- Neuron-Structure and ClassificationDokumen22 halamanNeuron-Structure and Classificationsunil patelBelum ada peringkat
- Deep Vein ThrombosisDokumen10 halamanDeep Vein Thrombosisزيد مسعودBelum ada peringkat
- Download ebook Duttons Orthopaedic Examination Evaluation And Intervention Pdf full chapter pdfDokumen67 halamanDownload ebook Duttons Orthopaedic Examination Evaluation And Intervention Pdf full chapter pdffrances.spencer341100% (21)
- BloodtransfusieDokumen79 halamanBloodtransfusieGod RaBelum ada peringkat
- Lesson17 Epithelial CellsDokumen22 halamanLesson17 Epithelial CellsGemma WrigleyBelum ada peringkat
- CTK-USA (Aria) : End User Price List-Rapid TestDokumen2 halamanCTK-USA (Aria) : End User Price List-Rapid TestAbdalazeez AlsayedBelum ada peringkat
- Penerapan Massage Effluerage Terhadap Penurunan Tekanan DarahDokumen7 halamanPenerapan Massage Effluerage Terhadap Penurunan Tekanan DarahindrinurmalasariBelum ada peringkat
- Drugs Use in HemostasisDokumen47 halamanDrugs Use in HemostasiskadibhaBelum ada peringkat
- Muscle TissueDokumen20 halamanMuscle TissueDheeraj MenezesBelum ada peringkat
- Abo Blood Group PDFDokumen17 halamanAbo Blood Group PDFIftikhar AhmadBelum ada peringkat
- Nervous TissueDokumen22 halamanNervous TissuePRIYA DARSHINI GUNALANBelum ada peringkat
- Blood Plasma Fractionation ProcessDokumen2 halamanBlood Plasma Fractionation ProcessAli Hussain100% (1)
- 1 SM PDFDokumen6 halaman1 SM PDFFina NABelum ada peringkat
- XN - Clinical Case - ReportDokumen83 halamanXN - Clinical Case - Report郑伟健Belum ada peringkat
- Blood Transfusion: Etiology of Blood CellDokumen4 halamanBlood Transfusion: Etiology of Blood Cellbunso padillaBelum ada peringkat