Anda mungkin juga menyukai
- A Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisDari EverandA Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisPenilaian: 3 dari 5 bintang3/5 (1)
- Anal Rectal DiseasesDokumen43 halamanAnal Rectal DiseasesNikita NababanBelum ada peringkat
- Anal Rectal DiseasesDokumen45 halamanAnal Rectal DiseasesAdhya TiaraBelum ada peringkat
- Pelvic Dysfunction in Men: Diagnosis and Treatment of Male Incontinence and Erectile DysfunctionDari EverandPelvic Dysfunction in Men: Diagnosis and Treatment of Male Incontinence and Erectile DysfunctionBelum ada peringkat
- Benign Anorectal Conditions: Ahmed Badrek-AmoudiDokumen20 halamanBenign Anorectal Conditions: Ahmed Badrek-AmoudiAna De La RosaBelum ada peringkat
- Bleeding Per RectumeDokumen35 halamanBleeding Per RectumetharakaBelum ada peringkat
- Anorectal DiseaseDokumen142 halamanAnorectal DiseaseAb Baby100% (1)
- Ano RectalDokumen57 halamanAno Rectaldrhemantt1279100% (1)
- PR BleedDokumen20 halamanPR BleedCathy KayBelum ada peringkat
- Hemor HoidDokumen22 halamanHemor HoidputyprilinaBelum ada peringkat
- Appendicitis - Dr. SigitDokumen50 halamanAppendicitis - Dr. SigitYuliana LatifBelum ada peringkat
- Grace Surgical HaemorrhoidDokumen4 halamanGrace Surgical HaemorrhoidBenny SuponoBelum ada peringkat
- Acute AbdomenDokumen36 halamanAcute AbdomenAdriani NadhirahBelum ada peringkat
- Acute Abdomen: - DefinitionDokumen27 halamanAcute Abdomen: - DefinitionWorku KifleBelum ada peringkat
- Anal Canal: Fissure in Ano HaemorrhoidsDokumen37 halamanAnal Canal: Fissure in Ano Haemorrhoidsyash shrivastavaBelum ada peringkat
- Pgi Hemorrhoids PresentationDokumen41 halamanPgi Hemorrhoids PresentationIkea BalhonBelum ada peringkat
- Appendicitis: DR - Sigid Djuniawan, SPBDokumen50 halamanAppendicitis: DR - Sigid Djuniawan, SPBWinda AlpiniawatiBelum ada peringkat
- Lower GIT BleedingDokumen30 halamanLower GIT BleedingRonald Joy DatuBelum ada peringkat
- HemorrhoidDokumen12 halamanHemorrhoidSasqia Trizolla0% (1)
- Introduction in UrologyDokumen69 halamanIntroduction in UrologyKaram SaadBelum ada peringkat
- Learning Objective: - Explain of Acute AbdomenDokumen143 halamanLearning Objective: - Explain of Acute AbdomenSamuel Sebastian SirapanjiBelum ada peringkat
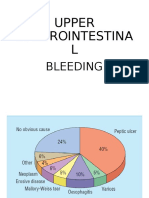
- Upper Gastrointestina L: BleedingDokumen35 halamanUpper Gastrointestina L: BleedingayuBelum ada peringkat
- Nursing Genito-Urinary SystemDokumen109 halamanNursing Genito-Urinary SystemKenny Nadela100% (1)
- RicoDokumen62 halamanRicoCunCunAlAndraBelum ada peringkat
- S13 Penyakit Dan Kelainan Sistem Gastrointestinal Dan Pankreatobilier Di Bidang BedahDokumen143 halamanS13 Penyakit Dan Kelainan Sistem Gastrointestinal Dan Pankreatobilier Di Bidang BedahDjamnur AgnessiaBelum ada peringkat
- Intestinal Obstruction: Ahmed Badrek-AmoudiDokumen26 halamanIntestinal Obstruction: Ahmed Badrek-Amoudiselvie87Belum ada peringkat
- Common Surgical PresentationsDokumen49 halamanCommon Surgical PresentationsJeremiah HiiBelum ada peringkat
- Differential Diagnosis of Flank PainDokumen43 halamanDifferential Diagnosis of Flank PainDrArish Mahmood78% (9)
- Peritoneum & Retroperit. Space DiseaseDokumen31 halamanPeritoneum & Retroperit. Space Diseasekaukab azimBelum ada peringkat
- Peritonitis: by Zziwa Hasim HassanDokumen17 halamanPeritonitis: by Zziwa Hasim Hassanstephen X-SILVERBelum ada peringkat
- 1100 Ultrasound of The Acute Abdomen 15 3Dokumen84 halaman1100 Ultrasound of The Acute Abdomen 15 3gp1promo2016Belum ada peringkat
- Management of Upper Gi BleedingDokumen41 halamanManagement of Upper Gi Bleedingkaukab azimBelum ada peringkat
- Abdominal Pain: Resources: Murtagh, John. General Practice 5 EdDokumen26 halamanAbdominal Pain: Resources: Murtagh, John. General Practice 5 EdDewanti PermatasariBelum ada peringkat
- Perdarahan Saluran CernaDokumen21 halamanPerdarahan Saluran CernaAmalia Hendar PangestutiBelum ada peringkat
- Urinary Hematologic Metabolic DisorderDokumen10 halamanUrinary Hematologic Metabolic DisorderGenki Fay B. LequiganBelum ada peringkat
- Back To Medical School: - Anorectal DisordersDokumen54 halamanBack To Medical School: - Anorectal DisordersSemSemBelum ada peringkat
- DR Wifanto S Jeo, SPB-BD - Acute AbdomenDokumen28 halamanDR Wifanto S Jeo, SPB-BD - Acute AbdomenIrma DamayantiBelum ada peringkat
- PERITONITISDokumen12 halamanPERITONITISHayat AL AKOUM100% (1)
- Anorectal DisordersDokumen59 halamanAnorectal DisordersdasdasfBelum ada peringkat
- Laporan Kasus - HemorrhoidsDokumen41 halamanLaporan Kasus - HemorrhoidsMetyana CahyaningtyasBelum ada peringkat
- Management of Malignant AscitesDokumen34 halamanManagement of Malignant Ascitesadaiah Soibi-HarryBelum ada peringkat
- Gi BleedingDokumen74 halamanGi Bleedingponcus payBelum ada peringkat
- Week2 LgitDokumen49 halamanWeek2 LgitriverabeanicoBelum ada peringkat
- Acute Abdominal Pain in ChildrenDokumen53 halamanAcute Abdominal Pain in ChildrenSutapa PawarBelum ada peringkat
- Bowel ObstructionDokumen48 halamanBowel ObstructionPatrick John100% (1)
- The Stomach and Duodenum: Dr. Elian EliasDokumen48 halamanThe Stomach and Duodenum: Dr. Elian EliasmodarBelum ada peringkat
- Abdominal Distention and AscitesDokumen49 halamanAbdominal Distention and AscitesNinaBelum ada peringkat
- 5c.BLEEDING ESOPHAGEAL VARICESDokumen11 halaman5c.BLEEDING ESOPHAGEAL VARICESHayat AL AKOUMBelum ada peringkat
- Gastrointestinal Bleeding: PCOM Internal Medicine Residents 2004Dokumen30 halamanGastrointestinal Bleeding: PCOM Internal Medicine Residents 2004nesakusumaBelum ada peringkat
- Renal and Urinary DisordersDokumen134 halamanRenal and Urinary Disordersmirmodepon05100% (1)
- Gynecology Case Discussion History & Clinical Examination: DR - Ketaki Junnare DR - Shweta DR - Priyadarshini Dr. NamrataDokumen36 halamanGynecology Case Discussion History & Clinical Examination: DR - Ketaki Junnare DR - Shweta DR - Priyadarshini Dr. Namratapriyadarshini adsulBelum ada peringkat
- ScrotalswellingDokumen82 halamanScrotalswellingNajihah MuhammadBelum ada peringkat
- Common Ward ProceduresDokumen27 halamanCommon Ward ProceduresZul Hisyam FikriBelum ada peringkat
- Acute AbdomenDokumen24 halamanAcute AbdomenGrace SimmonsBelum ada peringkat
- E. UrinaryDokumen16 halamanE. UrinaryGloryJaneBelum ada peringkat
- Urinary Tract InfectionDokumen27 halamanUrinary Tract InfectionNaseem Bin Yoosaf100% (1)
- GI Bleeding:: From Mouth To RectumDokumen31 halamanGI Bleeding:: From Mouth To RectumBendy Dwi IrawanBelum ada peringkat
- GI BleedDokumen28 halamanGI BleedAnn Lan100% (1)
- Urinary Disorders 2Dokumen19 halamanUrinary Disorders 2ula mdiBelum ada peringkat
- yZGn9p PaudelDokumen4 halamanyZGn9p PaudelAliyah Tofani PawelloiBelum ada peringkat
- Antibioprophylaxis: - Selective Gut DecontaminationDokumen30 halamanAntibioprophylaxis: - Selective Gut DecontaminationAliyah Tofani PawelloiBelum ada peringkat
- Benign Laryngeal Lesions Presentation TDuong 11-12-08Dokumen54 halamanBenign Laryngeal Lesions Presentation TDuong 11-12-08Aliyah Tofani PawelloiBelum ada peringkat
- Anatomy of BrainstemDokumen30 halamanAnatomy of BrainstemAliyah Tofani PawelloiBelum ada peringkat
- Definition and Etiology: PancreatitisDokumen24 halamanDefinition and Etiology: PancreatitisAliyah Tofani PawelloiBelum ada peringkat
- Pilonidal Sinus: Information For PatientsDokumen12 halamanPilonidal Sinus: Information For PatientsAliyah Tofani PawelloiBelum ada peringkat
- Acute Chronic PancreatitisDokumen38 halamanAcute Chronic PancreatitisAliyah Tofani PawelloiBelum ada peringkat
- Tumor Unknown Conference: June 2007Dokumen46 halamanTumor Unknown Conference: June 2007Aliyah Tofani PawelloiBelum ada peringkat
- A Seb Előadásom HonlapraDokumen52 halamanA Seb Előadásom HonlapraAliyah Tofani PawelloiBelum ada peringkat
- The Human Body: An OrientationDokumen35 halamanThe Human Body: An OrientationAliyah Tofani PawelloiBelum ada peringkat
- Anatomy and Physiology of The Gastrointestinal TractDokumen96 halamanAnatomy and Physiology of The Gastrointestinal TractAliyah Tofani PawelloiBelum ada peringkat
- 2304 UrinaryDokumen31 halaman2304 UrinaryAliyah Tofani PawelloiBelum ada peringkat
- Cystic Adenomatoid Malformation (CAM)Dokumen38 halamanCystic Adenomatoid Malformation (CAM)Aliyah Tofani PawelloiBelum ada peringkat
- Renal CystsDokumen28 halamanRenal CystsAliyah Tofani PawelloiBelum ada peringkat