Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Drug Calculations AssignmentDokumen2 halamanDrug Calculations AssignmentDarren RobertoBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Canadian Drug Names: Appendix EDokumen9 halamanCanadian Drug Names: Appendix EEmmanuel GaliciaBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grabovoi Numbers For HealingDokumen23 halamanGrabovoi Numbers For HealingAna BrunetteBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Mapeh 7-With TosDokumen5 halamanMapeh 7-With TosLorraine Calvez Donio100% (1)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
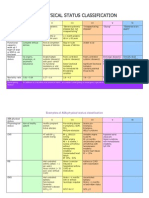
- Asa ClassDokumen3 halamanAsa ClassPriska Gusti Wulandari67% (3)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- 4 Asma Stepwise ApproachDokumen1 halaman4 Asma Stepwise ApproachbrianBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Amoxil: Amoxil Capsules 250 MG and 500 MG AmoxicillinDokumen7 halamanAmoxil: Amoxil Capsules 250 MG and 500 MG AmoxicillinrachbliBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- USFDA Approvals by CompanyDokumen136 halamanUSFDA Approvals by CompanyAsthaBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Breast and Nipple ConditionsDokumen23 halamanBreast and Nipple ConditionsdaveBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Physical Exam Report For New EmployeesDokumen1 halamanPhysical Exam Report For New Employeesirish xBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Pneumonii Curs AMG 2018Dokumen115 halamanPneumonii Curs AMG 2018Ionut Horgot100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Pharmaceutical Care Pasien Dengan Hipertensi Untuk Meningkatkan KualitasDokumen55 halamanPharmaceutical Care Pasien Dengan Hipertensi Untuk Meningkatkan KualitasREYNER AURELINUS MAXIMUS 2018Belum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Label ObatDokumen421 halamanLabel ObatjeanetBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- MenopauseDokumen53 halamanMenopauseShandy Suwanto PutraBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Co AmoxiclavDokumen1 halamanCo AmoxiclavMuhammad ArsalanBelum ada peringkat
- Genital Herpes: Aarthi (2012)Dokumen36 halamanGenital Herpes: Aarthi (2012)Aiman TymerBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rhinitis Allergic: Elma Wiliandini G4A020043Dokumen10 halamanRhinitis Allergic: Elma Wiliandini G4A020043elma wiliandiniBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
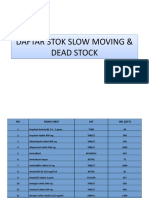
- Daftar Stok Slow Moving & Dead Stock Daftar Stok Slow Moving & Dead StockDokumen11 halamanDaftar Stok Slow Moving & Dead Stock Daftar Stok Slow Moving & Dead StockFebriyana SalehBelum ada peringkat
- Taking A Dermatological History - Dermatology - FastbleepDokumen5 halamanTaking A Dermatological History - Dermatology - Fastbleepkyle31Belum ada peringkat
- Immunization Requirements For Students in K12 in Texas 2018Dokumen4 halamanImmunization Requirements For Students in K12 in Texas 2018KCEN Channel 6Belum ada peringkat
- Abdominal Pain in ChildrenDokumen36 halamanAbdominal Pain in ChildrenKiani LarasBelum ada peringkat
- Burchum & Rosenthal: Lehne's Pharmacology For Nursing Care, 9th EditionDokumen7 halamanBurchum & Rosenthal: Lehne's Pharmacology For Nursing Care, 9th Editionhockeyman1584Belum ada peringkat
- Kode DiagnosaDokumen6 halamanKode DiagnosaRoy SuhendraBelum ada peringkat
- Physical Form 2018Dokumen2 halamanPhysical Form 2018api-247134277Belum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- تجميعةDokumen168 halamanتجميعةRn nadeenBelum ada peringkat
- HPV PowerpointDokumen11 halamanHPV PowerpointharyatikennitaBelum ada peringkat
- PICU Drug Handbook 2014 PDFDokumen106 halamanPICU Drug Handbook 2014 PDFMelissa SantosoBelum ada peringkat
- Label TabletDokumen9 halamanLabel TabletDedeh MahmudahBelum ada peringkat
- Case Study of LeptospirosisDokumen4 halamanCase Study of Leptospirosisbuzz Q75% (4)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- NSW Immunisation ScheduleDokumen1 halamanNSW Immunisation ScheduleKristinaBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)