Anda mungkin juga menyukai
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Approach To Pediatric AnemiaDokumen18 halamanApproach To Pediatric AnemiaMade Oka HeryanaBelum ada peringkat
- Normal Newborn PP Final-1Dokumen97 halamanNormal Newborn PP Final-1ettevyviBelum ada peringkat
- IMNCI Students' HandbookDokumen100 halamanIMNCI Students' HandbookGlaiza Marie D. GonzalesBelum ada peringkat
- Case StudyDokumen8 halamanCase Studybidisha06Belum ada peringkat
- Malnutritiom and Anemia ImciDokumen30 halamanMalnutritiom and Anemia ImcibaridacheBelum ada peringkat
- Abhay Jain Roll No 126Dokumen20 halamanAbhay Jain Roll No 126abhay jainBelum ada peringkat
- Competency Assessment Exam For Nurses: Qibah Hospital Qibah, Algassim, KsaDokumen4 halamanCompetency Assessment Exam For Nurses: Qibah Hospital Qibah, Algassim, KsaSherina W. Edding100% (1)
- 2 Assisting Clients To Use Incentive Spirometer DosdosDokumen3 halaman2 Assisting Clients To Use Incentive Spirometer DosdosBianca Mikaela DosdosBelum ada peringkat
- 6-Health Problems Common in PreschoolerDokumen36 halaman6-Health Problems Common in PreschoolerPam Lala100% (2)
- What Is LeadershipDokumen21 halamanWhat Is LeadershiptaapBelum ada peringkat
- 1 - Fetal Physiology and The Transition To Extrauterine LifeDokumen13 halaman1 - Fetal Physiology and The Transition To Extrauterine LifeRonaldo Pineda WieselbergBelum ada peringkat
- Miconium Aspiration SyndromeDokumen19 halamanMiconium Aspiration SyndromeEnna PaulaBelum ada peringkat
- Effectiveness of Structured Teaching Programme On Knowledge Regarding Prevention of Road Traffic Accidents Among Adolescents 13 18 Years in Selected Schools of Baramulla KashmirDokumen4 halamanEffectiveness of Structured Teaching Programme On Knowledge Regarding Prevention of Road Traffic Accidents Among Adolescents 13 18 Years in Selected Schools of Baramulla KashmirIJARP PublicationsBelum ada peringkat
- Acute Gastroenteritis FinalDokumen40 halamanAcute Gastroenteritis FinalAlbertina Aipinge NandjilaBelum ada peringkat
- An Interventional Study To Evaluate The Effectiveness of Selected Nutritional Diet On Growth of Pre Schooler at Selected Slums Area of Bhopal M.PDokumen6 halamanAn Interventional Study To Evaluate The Effectiveness of Selected Nutritional Diet On Growth of Pre Schooler at Selected Slums Area of Bhopal M.PEditor IJTSRDBelum ada peringkat
- Case Study On ResuscitationDokumen8 halamanCase Study On ResuscitationJasfer Guiao EnriquezBelum ada peringkat
- 144174d1376299459 Previous Years Question Papers Jipmer Staff Nurse Recruitment Exam Jipmer Question Paper 2012 PDFDokumen12 halaman144174d1376299459 Previous Years Question Papers Jipmer Staff Nurse Recruitment Exam Jipmer Question Paper 2012 PDFGaoudam NatarajanBelum ada peringkat
- Pediatric NursingDokumen4 halamanPediatric Nursingjustjesko0lBelum ada peringkat
- Enuresis in Children - A Case - Based ApproachDokumen9 halamanEnuresis in Children - A Case - Based ApproachBogdan NeamtuBelum ada peringkat
- Maternal and Child Heath: Jay Pee C. Malibiran Nurse 1 RNDokumen36 halamanMaternal and Child Heath: Jay Pee C. Malibiran Nurse 1 RNRosebel Lagura100% (1)
- Identification Data: A. Past Medical HistoryDokumen12 halamanIdentification Data: A. Past Medical HistoryPrernaSharmaBelum ada peringkat
- Cheat Sheet #92 - Disseminated Intravascular CoaguationDokumen3 halamanCheat Sheet #92 - Disseminated Intravascular CoaguationAsssBelum ada peringkat
- Kwashiorkor AND Marasmus: Group 6Dokumen18 halamanKwashiorkor AND Marasmus: Group 6Christian De GuzmanBelum ada peringkat
- Disseminated Intravascular Coagulation in Infants and Children - UpToDateDokumen16 halamanDisseminated Intravascular Coagulation in Infants and Children - UpToDateEduardo Romero Stéfani100% (2)
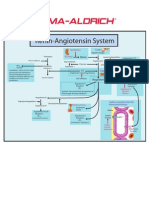
- Renin-Angiotensin SystemDokumen1 halamanRenin-Angiotensin SystemSigma-Aldrich100% (2)
- The Infection Control Manual: Standard PrecautionsDokumen5 halamanThe Infection Control Manual: Standard Precautionszenagit123456Belum ada peringkat
- Course Specification Emergency NursingDokumen6 halamanCourse Specification Emergency NursingWael LotfyBelum ada peringkat
- Child CPR: Skills Testing ChecklistDokumen3 halamanChild CPR: Skills Testing ChecklistTravis TravoltaBelum ada peringkat
- Paediatric Ophthalmology: DR Shuaibah Ab - Ghani Paediatric Ophthalmologist Hospital Queen Elizabeth Kota KinabaluDokumen41 halamanPaediatric Ophthalmology: DR Shuaibah Ab - Ghani Paediatric Ophthalmologist Hospital Queen Elizabeth Kota Kinabaluarnol3090Belum ada peringkat
- MeaslesDokumen32 halamanMeaslesYum C100% (2)
- Osh State UniversityDokumen14 halamanOsh State Universitykhuzaima9Belum ada peringkat
- About Rubella: VaccineDokumen5 halamanAbout Rubella: VaccinejudssalangsangBelum ada peringkat
- Urinary Retention PostpartumDokumen5 halamanUrinary Retention PostpartumpaswordnyalupaBelum ada peringkat
- Eye ExaminationDokumen23 halamanEye Examinationcynthia167Belum ada peringkat
- Nicu ReportDokumen66 halamanNicu ReportEr Shah Rukh QadriBelum ada peringkat
- Methods in Assessing Fetal Well-BeingDokumen27 halamanMethods in Assessing Fetal Well-BeingPasay Trisha Faye Y.Belum ada peringkat
- Newborn Disorders - : Small For Gestational Age (Sga) NewbornDokumen11 halamanNewborn Disorders - : Small For Gestational Age (Sga) Newborncayla mae carlos100% (1)
- Child With Blood Disorders PPT PRDokumen114 halamanChild With Blood Disorders PPT PRchaarviBelum ada peringkat
- Diagnosi S: MalariaDokumen28 halamanDiagnosi S: MalariaOm Prakash SinghBelum ada peringkat
- MeningitisDokumen12 halamanMeningitisFaith Vaughn100% (2)
- About Creamy LayerDokumen17 halamanAbout Creamy LayerbaluskbBelum ada peringkat
- Blood TransfusionDokumen5 halamanBlood TransfusionMoustafa Hazzaa100% (1)
- NCP Based On GordonsDokumen10 halamanNCP Based On GordonsFate Ann Candle Dagutao100% (1)
- Acute Stroke Nursing GuidelineFINAL 1 2Dokumen5 halamanAcute Stroke Nursing GuidelineFINAL 1 2radanikmaBelum ada peringkat
- Nephrotic SyndromeeDokumen28 halamanNephrotic SyndromeeRiteka SinghBelum ada peringkat
- Bone Marrow ChecklistDokumen2 halamanBone Marrow ChecklistHasyim SuparlanBelum ada peringkat
- Patient EducationDokumen14 halamanPatient EducationJ Therese NorrellBelum ada peringkat
- Drug Study: Francisco Tampos JRDokumen37 halamanDrug Study: Francisco Tampos JRCarlmeister Ambray JudillaBelum ada peringkat
- Neonatal SepsisDokumen17 halamanNeonatal SepsisDhilla Feroh Kesuma TBelum ada peringkat
- Cost EffectivenessDokumen22 halamanCost EffectivenessEdalyn CapiliBelum ada peringkat
- Assessment of NewbornDokumen26 halamanAssessment of Newbornaybee_14Belum ada peringkat
- Mechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeDokumen12 halamanMechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeGayathri RBelum ada peringkat
- Brain Tumor PDFDokumen11 halamanBrain Tumor PDFSujith KuttanBelum ada peringkat
- Renal FailureDokumen27 halamanRenal FailureMae DacerBelum ada peringkat
- Cardiac ArrythmiasDokumen37 halamanCardiac ArrythmiasRubina100% (1)
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesDari EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesBelum ada peringkat
- 2018 Article 61Dokumen11 halaman2018 Article 61gheaastridgayatriBelum ada peringkat
- Sar CodesDokumen6 halamanSar CodesnitkolBelum ada peringkat
- Med NotesDokumen277 halamanMed NotesSingey Lhendup100% (1)
- Neonatal HypotoniaDokumen7 halamanNeonatal HypotoniaShirley KoehBelum ada peringkat
- Daily Nursing AssessmentDokumen2 halamanDaily Nursing Assessmentkiku_laiBelum ada peringkat
- Administering Irrigation Eye Ear and NoseDokumen11 halamanAdministering Irrigation Eye Ear and NoseJan Federick BantayBelum ada peringkat
- Obesity and The Limits of Shame (2011)Dokumen174 halamanObesity and The Limits of Shame (2011)Ronnie RengiffoBelum ada peringkat
- Synthesis TranexamicDokumen6 halamanSynthesis TranexamicChính MùBelum ada peringkat
- Oral Anatomy DefinitionDokumen17 halamanOral Anatomy DefinitionJoe AjibadeBelum ada peringkat
- How Microorganism Cause DiseaseDokumen16 halamanHow Microorganism Cause DiseaseMARTINEZ JUSTINEBelum ada peringkat
- Cervical ColposDokumen6 halamanCervical ColposVictor DaminescuBelum ada peringkat
- Retrospective Study - The Presence of Malassezia in Feline Skin Biopsies. A Clinicopathological Study (Pages 7-14)Dokumen8 halamanRetrospective Study - The Presence of Malassezia in Feline Skin Biopsies. A Clinicopathological Study (Pages 7-14)jenBelum ada peringkat
- OB Hematologic DiseasesDokumen2 halamanOB Hematologic DiseasespreciousjemBelum ada peringkat
- Glycofilm - Solabia USA - 2011Dokumen7 halamanGlycofilm - Solabia USA - 2011Danielle BarkerBelum ada peringkat
- Nowak 2017Dokumen8 halamanNowak 2017Bogdan Marian SorohanBelum ada peringkat
- Isthmocele Uterin: A Propos de Quatre CasDokumen7 halamanIsthmocele Uterin: A Propos de Quatre CasIJAR JOURNALBelum ada peringkat
- Virus Web WorksheetDokumen3 halamanVirus Web WorksheetBrian Ramirez RamirezBelum ada peringkat
- Drug Study Hep BDokumen4 halamanDrug Study Hep BSawada TsunayoshiBelum ada peringkat
- Cerebral Palsy Practice Essentials: Signs and SymptomsDokumen11 halamanCerebral Palsy Practice Essentials: Signs and SymptomsTahsinur RahmanBelum ada peringkat
- Tchernof2013 PDFDokumen46 halamanTchernof2013 PDFindahBelum ada peringkat
- Additional Med CertDokumen1 halamanAdditional Med CertEmy MaquilingBelum ada peringkat
- Nbme 5.1Dokumen54 halamanNbme 5.1Hafsa SafdarBelum ada peringkat
- Brian A .Magowan - Part 2 SbasDokumen231 halamanBrian A .Magowan - Part 2 SbasAhmed Abdelgelil75% (4)
- The AVPU ScaleDokumen10 halamanThe AVPU ScalePrateek YadavBelum ada peringkat
- Quiz Process RecordingDokumen7 halamanQuiz Process RecordingDewley Guevarra MontenegroBelum ada peringkat
- Interdisciplinary Approach To The MandibDokumen7 halamanInterdisciplinary Approach To The MandibZachary DuongBelum ada peringkat
- OBMQ2 (3) Endocrine Diseases in Pregnancy - Dr. CandelarioDokumen8 halamanOBMQ2 (3) Endocrine Diseases in Pregnancy - Dr. Candelarioqsd clinicBelum ada peringkat
- Immuno 33 4 LinkedDokumen52 halamanImmuno 33 4 LinkedZuleynis MendozaBelum ada peringkat
- Intro To Virology NotesDokumen13 halamanIntro To Virology NotesSpongebob Squarepants100% (1)
- Bronchial Asthma: Harun ElçiçekDokumen54 halamanBronchial Asthma: Harun ElçiçekFiras Ali100% (2)