Anda mungkin juga menyukai
- My DiaryDokumen91 halamanMy DiarydrtgodeBelum ada peringkat
- Dosis Pemberian Obat Untuk Di Tempel Di ERDokumen6 halamanDosis Pemberian Obat Untuk Di Tempel Di ERHutomo 75Belum ada peringkat
- Bronchiolitis Assessment and Care PathwayDokumen2 halamanBronchiolitis Assessment and Care PathwaydrgrizahBelum ada peringkat
- Traffic Light SystemDokumen2 halamanTraffic Light SystemErick PrasetyaBelum ada peringkat
- Pediatrics Fluid and Electrolyte Maintenance CalculationDokumen26 halamanPediatrics Fluid and Electrolyte Maintenance CalculationAliaaBelum ada peringkat
- RUMAH SAKIT RM. 3.1 INSAN PERMATADokumen1 halamanRUMAH SAKIT RM. 3.1 INSAN PERMATADinaBelum ada peringkat
- Protocol of DehydrationDokumen3 halamanProtocol of DehydrationHamza El-ȜfifiBelum ada peringkat
- 04 - 3.2 - Pediatric EmergenciesDokumen149 halaman04 - 3.2 - Pediatric EmergenciesISFAHAN MASULOTBelum ada peringkat
- Index WayneDokumen4 halamanIndex WaynestellaBelum ada peringkat
- S1M3 Update Fluid Resuscitation Management in Emergency CasesDokumen70 halamanS1M3 Update Fluid Resuscitation Management in Emergency Casesgriya medicaBelum ada peringkat
- Rheumatology Case 1Dokumen6 halamanRheumatology Case 1ALMIRA GUANBelum ada peringkat
- Cerebrovascular Accident 14Dokumen33 halamanCerebrovascular Accident 14japheth01Belum ada peringkat
- Cerebrovascular Accident: AMA Computer Learning CenterDokumen33 halamanCerebrovascular Accident: AMA Computer Learning Centerhermesdave1100% (1)
- Sepsis Quick Reference GuideDokumen1 halamanSepsis Quick Reference GuideRavin DebieBelum ada peringkat
- Chapter 3 Coordination and ResponseDokumen22 halamanChapter 3 Coordination and ResponseNursaiyidah RoniBelum ada peringkat
- CPG - Acute Infectious DiarrheaDokumen52 halamanCPG - Acute Infectious DiarrheaJim Christian EllaserBelum ada peringkat
- What Is Fluid Therapy?Dokumen42 halamanWhat Is Fluid Therapy?Mirel YdianBelum ada peringkat
- Dehydration: DR Nadeem ZubairiDokumen78 halamanDehydration: DR Nadeem ZubairiDhitaBelum ada peringkat
- Physical AssessmentDokumen4 halamanPhysical AssessmentLouie ColladoBelum ada peringkat
- Formal Evaluation of Asthma Exacerbation Severity in The Urgent or Emergency CarDokumen3 halamanFormal Evaluation of Asthma Exacerbation Severity in The Urgent or Emergency Carمعاذ الشريفBelum ada peringkat
- Snakebite Severity Score Flowsheet Algorithm PDFDokumen2 halamanSnakebite Severity Score Flowsheet Algorithm PDFUmbu WindiBelum ada peringkat
- Is it COVID-19 or the flu? Check your symptomsDokumen1 halamanIs it COVID-19 or the flu? Check your symptomsDiyanaBelum ada peringkat
- Kuliah S2 AirDokumen23 halamanKuliah S2 AirViany RehansyahBelum ada peringkat
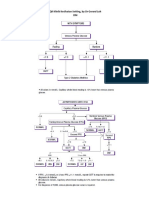
- QR Klinik Kesihatan Setting, by DR Gerard Loh DMDokumen34 halamanQR Klinik Kesihatan Setting, by DR Gerard Loh DMlailatul husnaBelum ada peringkat
- PQCNC CaroMont NAS Guide For FamiliesDokumen20 halamanPQCNC CaroMont NAS Guide For Familieskcochran100% (1)
- Table 2Dokumen1 halamanTable 2Anonymous TMUA6uUol9Belum ada peringkat
- Gen Notes Shock TableDokumen1 halamanGen Notes Shock TableAlenaBelum ada peringkat
- Critical Care Vital SignsDokumen29 halamanCritical Care Vital SignsPATHMAPRIYA GANESANBelum ada peringkat
- EMD2 - K8 - Acute Severe Asthma AttackDokumen34 halamanEMD2 - K8 - Acute Severe Asthma AttackJessica WijayaBelum ada peringkat
- Min Min Min Min: Most Urgent Very Urgent Urgent Less Urgent Not UrgentDokumen1 halamanMin Min Min Min: Most Urgent Very Urgent Urgent Less Urgent Not UrgentAlma Alnajjar0% (1)
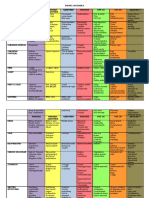
- Severity Change in TBW Change in ECF CV S/S Cns S/S Other S/S LabsDokumen2 halamanSeverity Change in TBW Change in ECF CV S/S Cns S/S Other S/S LabsGregBelum ada peringkat
- Body Fluid Compartments 0Dokumen15 halamanBody Fluid Compartments 0Abdo MohdyBelum ada peringkat
- New Snake EmergencyDokumen8 halamanNew Snake EmergencyRoxanneBelum ada peringkat
- SIADH Vs DI SN Study GuideDokumen1 halamanSIADH Vs DI SN Study Guidehvera01Belum ada peringkat
- Neurologi MANTAPDokumen154 halamanNeurologi MANTAPDita100% (2)
- Ultrasound Findings Reference Guide for Bladder, Pregnancy, Eye, FAST, Cardiac, Aorta, Bowel, Appendix, Pyloris, Gallbladder, Liver, Spleen, Pancreas, LungDokumen1 halamanUltrasound Findings Reference Guide for Bladder, Pregnancy, Eye, FAST, Cardiac, Aorta, Bowel, Appendix, Pyloris, Gallbladder, Liver, Spleen, Pancreas, LungRisa Anindia PutriBelum ada peringkat
- USReferenceValuesBasic PDFDokumen1 halamanUSReferenceValuesBasic PDFRisa Anindia PutriBelum ada peringkat
- Checking Vital Signs: Useful ExpressionDokumen2 halamanChecking Vital Signs: Useful ExpressionRatna PuspitaBelum ada peringkat
- Renal Anatomy, Physiology and Critical Care Concepts ExplainedDokumen25 halamanRenal Anatomy, Physiology and Critical Care Concepts ExplainedWaleed abdul hayeeBelum ada peringkat
- LGA 90th Percentile For GADokumen40 halamanLGA 90th Percentile For GAZimm RrrrBelum ada peringkat
- SEVERE DENGUEDokumen101 halamanSEVERE DENGUEtarakeeshbai1802Belum ada peringkat
- Palpation: Using The Sense of TouchDokumen54 halamanPalpation: Using The Sense of TouchAnna Fayeziah YussophBelum ada peringkat
- Clinical Assessment Mild Moderate Severe: Cultural Pulse PointsDokumen1 halamanClinical Assessment Mild Moderate Severe: Cultural Pulse PointsSanti PadmasariBelum ada peringkat
- Cga 1Dokumen37 halamanCga 1UDDE-E MARISABELBelum ada peringkat
- The ABC's in Pediatric Assessment and Care: Cymbeline Joan L. Pooten, RN NUM - Pediatric ICUDokumen39 halamanThe ABC's in Pediatric Assessment and Care: Cymbeline Joan L. Pooten, RN NUM - Pediatric ICUggrrk7Belum ada peringkat
- Classification by Gestational Age Preterm 42 WksDokumen46 halamanClassification by Gestational Age Preterm 42 WksAnna Fayeziah YussophBelum ada peringkat
- Mother & Baby Together Warm Room Fresh Clean Sheet/clothes Thermometer Weighing Scale Watch With Seconds StethoscopeDokumen50 halamanMother & Baby Together Warm Room Fresh Clean Sheet/clothes Thermometer Weighing Scale Watch With Seconds StethoscopeAnna Fayeziah YussophBelum ada peringkat
- Apgar Score: 0 1 2 1 Min 5 MinDokumen38 halamanApgar Score: 0 1 2 1 Min 5 MinZimm RrrrBelum ada peringkat
- Preceptor: Dr. Ihsanil Husna, Sp. PD: Arranged By: Rizki FebrianDokumen19 halamanPreceptor: Dr. Ihsanil Husna, Sp. PD: Arranged By: Rizki Febrianrizki febrianBelum ada peringkat
- Managing Dehydration and Electrolyte ImbalancesDokumen14 halamanManaging Dehydration and Electrolyte ImbalancesAzariah EbenezerBelum ada peringkat
- Brief CGA TemplateDokumen3 halamanBrief CGA TemplateMagister Keperawatan GerontikBelum ada peringkat
- Bowel Nosode MatrixDokumen3 halamanBowel Nosode MatrixKali KaliBelum ada peringkat
- Rotocol F Mergency Edicine: P OE MDokumen1 halamanRotocol F Mergency Edicine: P OE MKrishna ThakurBelum ada peringkat
- VelsamyDokumen7 halamanVelsamySivasubramanian BalasubramanianBelum ada peringkat
- Physical Examination (1) Basic Examination Techniques and General ExaminationDokumen9 halamanPhysical Examination (1) Basic Examination Techniques and General Examinationapi-19916399Belum ada peringkat
- Kegawatdaruratan IpdDokumen26 halamanKegawatdaruratan IpdSuci Nurul AmaliaBelum ada peringkat
- CroupDokumen20 halamanCroupFariezuan HamidBelum ada peringkat
- Dehydration PresentationDokumen27 halamanDehydration Presentationapi-352458054Belum ada peringkat
- Dehydration PresentationDokumen27 halamanDehydration Presentationapi-352458054Belum ada peringkat
- Dehydration PresentationDokumen27 halamanDehydration Presentationapi-352458054Belum ada peringkat
- Dehydration PresentationDokumen27 halamanDehydration Presentationapi-352458054Belum ada peringkat
- Dehydration PresentationDokumen27 halamanDehydration Presentationapi-352458054Belum ada peringkat