Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Moon Represents My HeartDokumen5 halamanThe Moon Represents My Heartchrissar1767% (3)
- The Moon Represents My HeartDokumen5 halamanThe Moon Represents My Heartchrissar1767% (3)
- The Moon Represents My HeartDokumen5 halamanThe Moon Represents My Heartchrissar1767% (3)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Aapd Guidelines - Restorative DentistryDokumen8 halamanAapd Guidelines - Restorative DentistrymahmoudBelum ada peringkat
- 4 5953781827192751296Dokumen119 halaman4 5953781827192751296Ridha Afzal100% (1)
- Coping With Stress Senior HighDokumen23 halamanCoping With Stress Senior HighJulienne Rose Penaranda Saballa100% (1)
- Survival Strategies For Parenting The Child & Teen With BipolarDokumen236 halamanSurvival Strategies For Parenting The Child & Teen With Bipolarseptiadhi wirawanBelum ada peringkat
- FINALS TheoreticalDokumen6 halamanFINALS TheoreticalCarol Neng Calupitan100% (1)
- NFDN 2007 Assignment 2Dokumen7 halamanNFDN 2007 Assignment 2api-287705803100% (2)
- Current Trends in PharmacovigilanceDokumen5 halamanCurrent Trends in PharmacovigilanceSutirtho MukherjiBelum ada peringkat
- Kodak Dental 1 Successful Panoramic RadiographyDokumen24 halamanKodak Dental 1 Successful Panoramic Radiographymanishbabu100% (2)
- Goal:: Ineffective Airway Clearance Related To Cumulation of SecretionDokumen4 halamanGoal:: Ineffective Airway Clearance Related To Cumulation of SecretionWyen CabatbatBelum ada peringkat
- Autorizacion CirugiaDokumen1 halamanAutorizacion Cirugiaanon_375322244Belum ada peringkat
- Job Duties of An Altar ServerDokumen4 halamanJob Duties of An Altar ServerAngie Lawrence100% (1)
- Standard Operation Procedure For First AidDokumen2 halamanStandard Operation Procedure For First AidAngie LawrenceBelum ada peringkat
- Venturer A5 Brochure PDFDokumen24 halamanVenturer A5 Brochure PDFAngie LawrenceBelum ada peringkat
- Altar Server Form 2 With Sepcial OcassionDokumen4 halamanAltar Server Form 2 With Sepcial OcassionAngie LawrenceBelum ada peringkat
- AbdomenDokumen55 halamanAbdomenAngie LawrenceBelum ada peringkat
- BiYe Kaoshi - Grade 2009 Single Choice QuestionsDokumen7 halamanBiYe Kaoshi - Grade 2009 Single Choice QuestionsAngie LawrenceBelum ada peringkat
- BiYe Kaoshi - Grade 2009 Single Choice QuestionsDokumen7 halamanBiYe Kaoshi - Grade 2009 Single Choice QuestionsAngie LawrenceBelum ada peringkat
- Chapter Four-Qi, Blood, Body FluidDokumen34 halamanChapter Four-Qi, Blood, Body FluidAngie LawrenceBelum ada peringkat
- Epidemic Cerebrospinal MeningitisDokumen76 halamanEpidemic Cerebrospinal MeningitisAngie LawrenceBelum ada peringkat
- Power To Persevere 5 Lessons - MarkDokumen10 halamanPower To Persevere 5 Lessons - MarkAngie LawrenceBelum ada peringkat
- General Intercessions 30 Nov 2014Dokumen1 halamanGeneral Intercessions 30 Nov 2014Angie LawrenceBelum ada peringkat
- Lit Planning Guide Baptism Outside Mass 112711Dokumen4 halamanLit Planning Guide Baptism Outside Mass 112711Angie LawrenceBelum ada peringkat
- Quiz Chapter 6 ANSDokumen2 halamanQuiz Chapter 6 ANSAngie LawrenceBelum ada peringkat
- Revision Timetable Example 4 PDFDokumen1 halamanRevision Timetable Example 4 PDFAngie LawrenceBelum ada peringkat
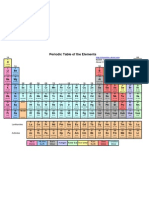
- Periodic Table All ColorDokumen1 halamanPeriodic Table All ColorcingggggggggggBelum ada peringkat
- USMLE World Behavioral ScienceDokumen179 halamanUSMLE World Behavioral ScienceAngie Lawrence100% (1)
- A Taste of SoutheastDokumen10 halamanA Taste of SoutheastAngie LawrenceBelum ada peringkat
- Revision Timetable Example 4 PDFDokumen1 halamanRevision Timetable Example 4 PDFAngie LawrenceBelum ada peringkat
- QPFamily Feud InstrDokumen48 halamanQPFamily Feud InstrAngie LawrenceBelum ada peringkat
- Title: Experiment 1 Techniques of Using Microscope Student'S Name: Angie Lawrence Student'S Id: CPM13/12DDokumen6 halamanTitle: Experiment 1 Techniques of Using Microscope Student'S Name: Angie Lawrence Student'S Id: CPM13/12DAngie LawrenceBelum ada peringkat
- DNA Replication: Meselson & Stahl's Semiconservative ExperimentDokumen4 halamanDNA Replication: Meselson & Stahl's Semiconservative ExperimentAngie LawrenceBelum ada peringkat
- Nursing Care Plan for a Client with Acute Gouty ArthritisDokumen4 halamanNursing Care Plan for a Client with Acute Gouty ArthritisTikTok TrendzBelum ada peringkat
- Shock Power PointDokumen24 halamanShock Power PointmarwaBelum ada peringkat
- Saint Alphonsus Statement On LettersDokumen1 halamanSaint Alphonsus Statement On LettersKBOI 2NewsBelum ada peringkat
- Nurs402 Teachingprojectsummary NeuburgDokumen20 halamanNurs402 Teachingprojectsummary Neuburgapi-452041818Belum ada peringkat
- Coley 2019Dokumen8 halamanColey 2019KaniBelum ada peringkat
- Jurnal Insect Bite PDFDokumen4 halamanJurnal Insect Bite PDFjihadahBelum ada peringkat
- Chronic Suppurative Otitis MediaDokumen4 halamanChronic Suppurative Otitis MediarchristoverBelum ada peringkat
- AllDokumen48 halamanAllnanchieBelum ada peringkat
- EBM Research DesignDokumen107 halamanEBM Research DesignAdhika WijayantiBelum ada peringkat
- AplDokumen37 halamanApladitiya tegarBelum ada peringkat
- Handout Knight in Rusty ArmourDokumen9 halamanHandout Knight in Rusty ArmourGobetiBelum ada peringkat
- Calista Roy LuigiDokumen22 halamanCalista Roy LuigiLuigi Prada GuzmanBelum ada peringkat
- MIASMS THE REAL TRACK TO CUREDokumen5 halamanMIASMS THE REAL TRACK TO CUREjiurgiuBelum ada peringkat
- Treatment Metastatic Ca ColonDokumen9 halamanTreatment Metastatic Ca ColonBurhan MinervaBelum ada peringkat
- Freud Constructions in AnalysisDokumen9 halamanFreud Constructions in AnalysisyaelfridBelum ada peringkat
- Assessing Body TemperatureDokumen6 halamanAssessing Body TemperatureemailBelum ada peringkat
- ArrowDokumen12 halamanArrowcelestialionBelum ada peringkat
- Medrano Neuro Notes 2.0Dokumen22 halamanMedrano Neuro Notes 2.0roldan pantojaBelum ada peringkat
- Newcastle Satisfaction With Nursing Scales AnDokumen6 halamanNewcastle Satisfaction With Nursing Scales AnlemootpBelum ada peringkat
- Code of Conduct EnglishDokumen8 halamanCode of Conduct EnglishNithya NambiarBelum ada peringkat