Anda mungkin juga menyukai
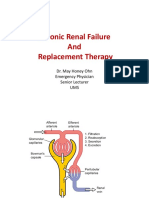
- Chronic Renal Failure and Renal Replacement TherapyDokumen76 halamanChronic Renal Failure and Renal Replacement TherapyMohd Johari Mohd ShafuwanBelum ada peringkat
- 2016 PE2 TheoryDokumen21 halaman2016 PE2 TheoryMohd Johari Mohd ShafuwanBelum ada peringkat
- Chest Tube, Urinary Catheter, Ryles Tube InsertionDokumen60 halamanChest Tube, Urinary Catheter, Ryles Tube InsertionMohd Johari Mohd ShafuwanBelum ada peringkat
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisDokumen35 halamanLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanBelum ada peringkat
- Antibiotics (Role and Abuse) 2016Dokumen35 halamanAntibiotics (Role and Abuse) 2016Mohd Johari Mohd ShafuwanBelum ada peringkat
- Connective Tissue DiseasesDokumen22 halamanConnective Tissue DiseasesMohd Johari Mohd ShafuwanBelum ada peringkat
- l8 Management of Perianal Pain and ConditionsDokumen51 halamanl8 Management of Perianal Pain and ConditionsMohd Johari Mohd ShafuwanBelum ada peringkat
- Abg InterpretationDokumen1 halamanAbg InterpretationMohd Johari Mohd ShafuwanBelum ada peringkat
- Antibiotics (Role and Abuse)Dokumen35 halamanAntibiotics (Role and Abuse)Mohd Johari Mohd ShafuwanBelum ada peringkat
- Health Promotion LO1&2Dokumen24 halamanHealth Promotion LO1&2Mohd Johari Mohd ShafuwanBelum ada peringkat
- PruritusDokumen9 halamanPruritusMohd Johari Mohd ShafuwanBelum ada peringkat
- Health Promotion LO4Dokumen41 halamanHealth Promotion LO4Mohd Johari Mohd ShafuwanBelum ada peringkat
- Acute Liver FailureDokumen24 halamanAcute Liver FailureMohd Johari Mohd ShafuwanBelum ada peringkat
- SGD 10Dokumen38 halamanSGD 10Mohd Johari Mohd ShafuwanBelum ada peringkat
- Adult Immunisation Guideline 2nd Edition 2014Dokumen184 halamanAdult Immunisation Guideline 2nd Edition 2014Mohd Johari Mohd ShafuwanBelum ada peringkat
- Childhood Immunization OWDokumen24 halamanChildhood Immunization OWMohd Johari Mohd ShafuwanBelum ada peringkat
- Avascular NecrosisDokumen41 halamanAvascular NecrosisMohd Johari Mohd Shafuwan100% (1)
- Open FracturesDokumen43 halamanOpen FracturesMohd Johari Mohd ShafuwanBelum ada peringkat
- Case Presentation 2Dokumen42 halamanCase Presentation 2Mohd Johari Mohd ShafuwanBelum ada peringkat
- Lo 5 and 6Dokumen32 halamanLo 5 and 6Mohd Johari Mohd ShafuwanBelum ada peringkat
- New AsiaDokumen2 halamanNew AsiaMónica CruzBelum ada peringkat
- SchizophreniaDokumen67 halamanSchizophreniaHazirah Mokhtar100% (1)
- l8 Diabetes Melitus in PregnancyDokumen23 halamanl8 Diabetes Melitus in PregnancyMohd Johari Mohd ShafuwanBelum ada peringkat
- Diabetes Mellitus in District HospitalDokumen30 halamanDiabetes Mellitus in District HospitalMohd Johari Mohd ShafuwanBelum ada peringkat
- Normal ECGDokumen63 halamanNormal ECGMohd Johari Mohd ShafuwanBelum ada peringkat
- Ecg Basics Part 1Dokumen78 halamanEcg Basics Part 1Mohd Johari Mohd ShafuwanBelum ada peringkat
- Dengue Fever in Malaysia - Fadhila & NadiahDokumen11 halamanDengue Fever in Malaysia - Fadhila & NadiahJacklyn NgBelum ada peringkat
- CPG - Unstable Angina-NSTEMIDokumen62 halamanCPG - Unstable Angina-NSTEMIMohd RafiBelum ada peringkat
- Malignant Bone Tumours and Staging of MSK TumourDokumen30 halamanMalignant Bone Tumours and Staging of MSK TumourMohd Johari Mohd ShafuwanBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Message To St. MatthewDokumen3 halamanMessage To St. MatthewAlvin MotillaBelum ada peringkat
- Incremental Analysis 2Dokumen12 halamanIncremental Analysis 2enter_sas100% (1)
- Edu 536 - Task A2 - pld5Dokumen3 halamanEdu 536 - Task A2 - pld5api-281740174Belum ada peringkat
- BreadTalk - Annual Report 2014Dokumen86 halamanBreadTalk - Annual Report 2014Vicky NeoBelum ada peringkat
- Assignment 1 TVM, Bonds StockDokumen2 halamanAssignment 1 TVM, Bonds StockMuhammad Ali SamarBelum ada peringkat
- Dances in LuzonDokumen13 halamanDances in LuzonDenise Michelle AntivoBelum ada peringkat
- K Unit 1 SeptemberDokumen2 halamanK Unit 1 Septemberapi-169447826Belum ada peringkat
- SANCHEZ V DEMETRIOUDokumen3 halamanSANCHEZ V DEMETRIOUShenna SunicoBelum ada peringkat
- Walmart Assignment1Dokumen13 halamanWalmart Assignment1kingkammyBelum ada peringkat
- 145class 7 Integers CH 1Dokumen2 halaman145class 7 Integers CH 17A04Aditya MayankBelum ada peringkat
- Jack Pumpkinhead of Oz - L. Frank BaumDokumen68 halamanJack Pumpkinhead of Oz - L. Frank BaumbobbyejayneBelum ada peringkat
- PRS Product DescriptionDokumen42 halamanPRS Product DescriptioneliaezekielBelum ada peringkat
- Deborah Schiffrin .Tense Variation in NarrativeDokumen19 halamanDeborah Schiffrin .Tense Variation in Narrativealwan61Belum ada peringkat
- Health Assessment Finals Review Flashcards - QuizletDokumen92 halamanHealth Assessment Finals Review Flashcards - QuizletViea Pacaco SivaBelum ada peringkat
- Semi-Detailed Lesson Plan in Tle (Cookery) Mhaylani O. Otanes-Flores 1 February 16, 2022 (Wednesday) 7 TLE-Cookery 1 10Dokumen4 halamanSemi-Detailed Lesson Plan in Tle (Cookery) Mhaylani O. Otanes-Flores 1 February 16, 2022 (Wednesday) 7 TLE-Cookery 1 10Mhaylani Otanes100% (1)
- Wardancer 4e HomebrewDokumen3 halamanWardancer 4e HomebrewWyjecBelum ada peringkat
- BA BBA Law of Crimes II CRPC SEM IV - 11Dokumen6 halamanBA BBA Law of Crimes II CRPC SEM IV - 11krish bhatia100% (1)
- Emcee - Graduation DayDokumen5 halamanEmcee - Graduation DayBharanisri VeerendiranBelum ada peringkat
- MCQ On ErgonomicsDokumen4 halamanMCQ On Ergonomicszoom milind67% (3)
- Parathyroid Agents PDFDokumen32 halamanParathyroid Agents PDFRhodee Kristine DoñaBelum ada peringkat
- If He Asked YouDokumen10 halamanIf He Asked YouLourdes MartinsBelum ada peringkat
- Pakistan's Professor Mafia - Pakistan - DAWNDokumen5 halamanPakistan's Professor Mafia - Pakistan - DAWNMuhammad Bilal A. RBelum ada peringkat
- A Palace in TimeDokumen6 halamanA Palace in TimeSonkheBelum ada peringkat
- Project Report: Eveplus Web PortalDokumen47 halamanProject Report: Eveplus Web Portaljas121Belum ada peringkat
- S.I.M. InnovaDokumen51 halamanS.I.M. InnovaPauline Karen ConcepcionBelum ada peringkat
- Neuralink DocumentationDokumen25 halamanNeuralink DocumentationVAIDIK Kasoju100% (6)
- PSYCHODYNAMICS AND JUDAISM The Jewish in Uences in Psychoanalysis and Psychodynamic TheoriesDokumen33 halamanPSYCHODYNAMICS AND JUDAISM The Jewish in Uences in Psychoanalysis and Psychodynamic TheoriesCarla MissionaBelum ada peringkat
- Comparative Analysis of Levis Wrangler & LeeDokumen10 halamanComparative Analysis of Levis Wrangler & LeeNeelakshi srivastavaBelum ada peringkat
- Ritual 2 Turning Attraction Into LoveDokumen2 halamanRitual 2 Turning Attraction Into Lovekrlup0% (1)
- Practice Test 12 Use of English I. Choose The Best AnswerDokumen6 halamanPractice Test 12 Use of English I. Choose The Best AnswerJack NguyễnBelum ada peringkat