Anda mungkin juga menyukai
- Modern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.Dari EverandModern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.Belum ada peringkat
- ER 23-24 Juli 2016Dokumen55 halamanER 23-24 Juli 2016Theresia Alfionita SinulinggaBelum ada peringkat
- TN MahyuniDokumen16 halamanTN MahyuniJacky JunaediBelum ada peringkat
- Emergency Report January 10-11 2017: Chief On Duty: Coass On DutyDokumen83 halamanEmergency Report January 10-11 2017: Chief On Duty: Coass On DutyYulianti Yulianti YuliantiBelum ada peringkat
- Emergency Case TemplateDokumen16 halamanEmergency Case TemplateJacky JunaediBelum ada peringkat
- Emergency Report: July 26 - July 27 2016Dokumen40 halamanEmergency Report: July 26 - July 27 2016Theresia Alfionita SinulinggaBelum ada peringkat
- Obscure Gastrointestinal Bleeding: Chylous AscitesDokumen2 halamanObscure Gastrointestinal Bleeding: Chylous AscitesMintdonBelum ada peringkat
- Emergency Case Report 4 - 5 February 2019: TH THDokumen49 halamanEmergency Case Report 4 - 5 February 2019: TH THmonyet65Belum ada peringkat
- Dynamic Practice Guidelines For Emergency General SurgeryDokumen19 halamanDynamic Practice Guidelines For Emergency General SurgeryJolaine ValloBelum ada peringkat
- Emergency: Case ReportDokumen63 halamanEmergency: Case Reporttania jannahBelum ada peringkat
- Concept Map 10 25 23 RachelDokumen1 halamanConcept Map 10 25 23 Rachelapi-726698459Belum ada peringkat
- Cholecystectomy Data and Case ScenarioDokumen14 halamanCholecystectomy Data and Case ScenarioJames Conrad SalengaBelum ada peringkat
- Emergency: Case ReportDokumen63 halamanEmergency: Case Reporttania jannahBelum ada peringkat
- KARDEX (Admission)Dokumen1 halamanKARDEX (Admission)JA BerzabalBelum ada peringkat
- EMERGENCY REPORT: 9 PATIENTS TREATED FOR INJURIES AND ILLNESSESDokumen96 halamanEMERGENCY REPORT: 9 PATIENTS TREATED FOR INJURIES AND ILLNESSESZakkyMaulanaRahmatBelum ada peringkat
- KARDEX (Admission)Dokumen1 halamanKARDEX (Admission)JA BerzabalBelum ada peringkat
- PREOPinguinalherniaDokumen2 halamanPREOPinguinalherniapatriciaatan1497Belum ada peringkat
- Emergency Case Report June 8 - 9 2019: TH THDokumen83 halamanEmergency Case Report June 8 - 9 2019: TH THEmma AssagafBelum ada peringkat
- Macabali GS2Dokumen4 halamanMacabali GS2Christian Edward MacabaliBelum ada peringkat
- Course in The Wards FormatDokumen2 halamanCourse in The Wards FormatJade MonrealBelum ada peringkat
- Friday 4-5-2018 HematocheziaDokumen20 halamanFriday 4-5-2018 HematocheziaJefri SusantoBelum ada peringkat
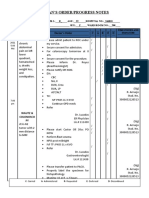
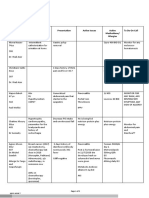
- Date Progress Notes Doctor's Order C AR E DDokumen4 halamanDate Progress Notes Doctor's Order C AR E DRenea Joy ArruejoBelum ada peringkat
- 10 31 Concept MapDokumen1 halaman10 31 Concept Mapapi-725271439Belum ada peringkat
- Laporan Jaga Igd: Rsud Adhiyatma, MPH Coass Bedah UnimusDokumen27 halamanLaporan Jaga Igd: Rsud Adhiyatma, MPH Coass Bedah UnimusDony Hamonangan SiregarBelum ada peringkat
- Surgery PearlsDokumen2 halamanSurgery Pearlspatriciaatan1497Belum ada peringkat
- Sample ChartingDokumen1 halamanSample ChartingAnn Justine OrbetaBelum ada peringkat
- Handoff Note 13-7-2020Dokumen2 halamanHandoff Note 13-7-2020Ali El SafadiBelum ada peringkat
- Handoff Note 13-7-2020!!!!Dokumen2 halamanHandoff Note 13-7-2020!!!!Ali El SafadiBelum ada peringkat
- Surgery PearlsDokumen2 halamanSurgery Pearlspatriciaatan1497Belum ada peringkat
- 189 Gotera, Chloe Lynn - HPS DAY 2Dokumen7 halaman189 Gotera, Chloe Lynn - HPS DAY 2Chloe GoteraBelum ada peringkat
- Left Side Appendix With Appendicitis 333Dokumen3 halamanLeft Side Appendix With Appendicitis 333Medtext PublicationsBelum ada peringkat
- Table 1: Intial Evaluation On Arrival To ER For All PatientsDokumen1 halamanTable 1: Intial Evaluation On Arrival To ER For All PatientsHetoshima KeiBelum ada peringkat
- PBL - CardioDokumen5 halamanPBL - Cardiogie sarcedaBelum ada peringkat
- Peptic Ulcer Concept MapDokumen17 halamanPeptic Ulcer Concept MappotchistroberriBelum ada peringkat
- Morning Report Details Gastrointestinal Bleeding CaseDokumen25 halamanMorning Report Details Gastrointestinal Bleeding CasePramudia DeniBelum ada peringkat
- HIS DataDokumen2 halamanHIS DataAhmed AbuelezzBelum ada peringkat
- Caeco-peritoneal band: an overlooked cause of chronic right iliac fossa pain in childrenDokumen5 halamanCaeco-peritoneal band: an overlooked cause of chronic right iliac fossa pain in childrenIoannis ValioulisBelum ada peringkat
- New Intern Guide Quick NotesDokumen8 halamanNew Intern Guide Quick NotesTrisBelum ada peringkat
- PDF Nursing Care PlanDokumen16 halamanPDF Nursing Care PlanMichael MabiniBelum ada peringkat
- Is It An Acute Pain Transfusion Reaction?: Case ReportDokumen3 halamanIs It An Acute Pain Transfusion Reaction?: Case ReportDr KalyanBelum ada peringkat
- Slide MR 7 - 8 Agustus 2017Dokumen62 halamanSlide MR 7 - 8 Agustus 2017Heru WahyudiBelum ada peringkat
- Acute Mesenteric Ischaemia on Unenhanced CTDokumen7 halamanAcute Mesenteric Ischaemia on Unenhanced CTmike_lavaresBelum ada peringkat
- nsg-320 Careplan 3Dokumen8 halamannsg-320 Careplan 3api-521051373Belum ada peringkat
- Intestinal Obstruction Due To PostDokumen8 halamanIntestinal Obstruction Due To PostSelene CotardoBelum ada peringkat
- Appendiceal Hernia: An Extremely Rare Condition: Online Case ReportDokumen3 halamanAppendiceal Hernia: An Extremely Rare Condition: Online Case ReportGabriel MolinaBelum ada peringkat
- Concept MapDokumen14 halamanConcept Mapapi-419091662Belum ada peringkat
- Course in The Ward: Date and Time Focus Doctor's Order Nurses Note August 28, 2018 3:50PM Vital Signs: AdmissionDokumen4 halamanCourse in The Ward: Date and Time Focus Doctor's Order Nurses Note August 28, 2018 3:50PM Vital Signs: AdmissionMartin T ManuelBelum ada peringkat
- Kim Johnson's Medical ChartDokumen13 halamanKim Johnson's Medical ChartFranz Patrick Legria, CPAC - SNBelum ada peringkat
- Perdarahan Saluran Cerna Bagian BawahDokumen33 halamanPerdarahan Saluran Cerna Bagian BawahGiyani LiberthiBelum ada peringkat
- Nefrologi: I Gusti Ngurah Agung Tresna ErawanDokumen69 halamanNefrologi: I Gusti Ngurah Agung Tresna ErawanDian PritaBelum ada peringkat
- Resume: Hyperthyroid Perioperative ManagementDokumen4 halamanResume: Hyperthyroid Perioperative ManagementWilujeng AnggrainiBelum ada peringkat
- Suggested Algorithm For Patients With Acute Upper .: BleedingDokumen4 halamanSuggested Algorithm For Patients With Acute Upper .: BleedingMimi Marjorie TecBelum ada peringkat
- Scribe America Final, Emergency DepartmentDokumen41 halamanScribe America Final, Emergency DepartmentJulio CastilloBelum ada peringkat
- Ozan MR Ny Rusmini Dan SUIB-fixDokumen21 halamanOzan MR Ny Rusmini Dan SUIB-fixahmadfauzanarifaniBelum ada peringkat
- Common Abbreviations For The Patient Note USMLE Step 2CSDokumen1 halamanCommon Abbreviations For The Patient Note USMLE Step 2CSTiondi francisBelum ada peringkat
- Medication Mechanism of Action Indications Contraindications Side Effects Nursing ResponsibilitiesDokumen1 halamanMedication Mechanism of Action Indications Contraindications Side Effects Nursing Responsibilitiesjoan bagnateBelum ada peringkat
- Things To Look For During Morning RoundDokumen3 halamanThings To Look For During Morning RoundTom YipBelum ada peringkat
- Emergency: Chief On Duty: Yuli Coass On Duty: Akbar, Febri, FauzanDokumen28 halamanEmergency: Chief On Duty: Yuli Coass On Duty: Akbar, Febri, FauzanahmadfauzanarifaniBelum ada peringkat
- Surgery BoardsDokumen16 halamanSurgery Boardscusom34100% (1)
- Acute Medicine: Shock: Inadequate Tissue and Organ PerfusionDokumen3 halamanAcute Medicine: Shock: Inadequate Tissue and Organ Perfusionmyat252Belum ada peringkat
- Oral Cancer Diagnosis and TherapyDokumen427 halamanOral Cancer Diagnosis and TherapyJacky Junaedi100% (2)
- Muenke PaperDokumen7 halamanMuenke PaperJacky JunaediBelum ada peringkat
- 10 1001@jama 2016 0287Dokumen10 halaman10 1001@jama 2016 0287ompardor7554Belum ada peringkat
- Athraa A. Mahmood M.Sc. of Periodontics: Prepared byDokumen22 halamanAthraa A. Mahmood M.Sc. of Periodontics: Prepared byJacky JunaediBelum ada peringkat
- InfectionDokumen45 halamanInfectionJacky JunaediBelum ada peringkat
- Pathfast BrochureDokumen6 halamanPathfast BrochureJacky Junaedi100% (1)
- Determination of Reference Interval For Presepsin, An Early Marker For Sepsis - Biochemia MedicaDokumen5 halamanDetermination of Reference Interval For Presepsin, An Early Marker For Sepsis - Biochemia MedicaJacky JunaediBelum ada peringkat
- VictoriaSchunemann ApertSyndromeDokumen27 halamanVictoriaSchunemann ApertSyndromeJacky JunaediBelum ada peringkat
- 1 Hochman NYSDJDokumen6 halaman1 Hochman NYSDJJacky JunaediBelum ada peringkat
- A Case of Sepsis Caused by Odontogenic Infection With Temporal Fossa and Pericostal AbscessDokumen1 halamanA Case of Sepsis Caused by Odontogenic Infection With Temporal Fossa and Pericostal AbscessJacky JunaediBelum ada peringkat
- Dental Flap DesignDokumen31 halamanDental Flap Designgeethagm4Belum ada peringkat
- 6 Surgical Periodontal TherapyDokumen38 halaman6 Surgical Periodontal TherapyPriya SargunanBelum ada peringkat
- Peripheral Cemento-Ossifying Fibroma of MaxillaDokumen11 halamanPeripheral Cemento-Ossifying Fibroma of MaxillaJacky JunaediBelum ada peringkat
- Manual Abx055370Dokumen4 halamanManual Abx055370Jacky JunaediBelum ada peringkat
- Odontogenic Infections For SeminarDokumen11 halamanOdontogenic Infections For SeminarJacky JunaediBelum ada peringkat
- Piis0901502717314777 2Dokumen9 halamanPiis0901502717314777 2Jacky JunaediBelum ada peringkat
- Prognostic Scoring Systems and Outcome Markers in ICU PatientsDokumen2 halamanPrognostic Scoring Systems and Outcome Markers in ICU PatientsJacky JunaediBelum ada peringkat
- PROSPEKT ENG Presepsin Time Is Survival ID 6153Dokumen15 halamanPROSPEKT ENG Presepsin Time Is Survival ID 6153Jacky JunaediBelum ada peringkat
- Presepsin FinalDokumen5 halamanPresepsin FinalJacky JunaediBelum ada peringkat
- Pre Album inDokumen5 halamanPre Album inJacky JunaediBelum ada peringkat
- Contemporary Oral Oncology Diagnosis and ManagementDokumen327 halamanContemporary Oral Oncology Diagnosis and ManagementJacky JunaediBelum ada peringkat
- Dermoid cysts of the floor of the mouth: case report and literature reviewDokumen1 halamanDermoid cysts of the floor of the mouth: case report and literature reviewJacky JunaediBelum ada peringkat
- Bang Hendi 3Dokumen10 halamanBang Hendi 3Jacky JunaediBelum ada peringkat
- Ranula: A Review of LiteratureDokumen6 halamanRanula: A Review of LiteratureNicco MarantsonBelum ada peringkat
- Sanggar BorneoDokumen1 halamanSanggar BorneoJacky JunaediBelum ada peringkat
- TN NgadinoDokumen16 halamanTN NgadinoJacky JunaediBelum ada peringkat
- Tennison Type Lip Repair PDFDokumen7 halamanTennison Type Lip Repair PDFJacky JunaediBelum ada peringkat
- Disorder of Circulation, Body Fluid and BasicDokumen65 halamanDisorder of Circulation, Body Fluid and BasicJacky JunaediBelum ada peringkat
- Emergency Case TemplateDokumen46 halamanEmergency Case TemplateJacky JunaediBelum ada peringkat
- TN ErwinDokumen13 halamanTN ErwinJacky JunaediBelum ada peringkat
- Bacillus lipopeptides: versatile weapons against plant diseasesDokumen11 halamanBacillus lipopeptides: versatile weapons against plant diseasesjazminBelum ada peringkat
- Zoology: Zoology Previous Eamcet QuestionsDokumen8 halamanZoology: Zoology Previous Eamcet QuestionsGaganpreetSingh100% (1)
- First Layer Coursera Learning How To LearnDokumen4 halamanFirst Layer Coursera Learning How To LearnSandy SharmaBelum ada peringkat
- Haemoglobin: DR Nilesh Kate MBBS, MD Associate ProfDokumen31 halamanHaemoglobin: DR Nilesh Kate MBBS, MD Associate ProfMarcellia100% (1)
- GEC General Studies Part 1Dokumen42 halamanGEC General Studies Part 1daisyBelum ada peringkat
- MRCP 2 Nephrology NOTESDokumen74 halamanMRCP 2 Nephrology NOTESMuhammad HaneefBelum ada peringkat
- Comparative Study The Effect of Induction of General Anesthesia With Propofol Versus Thiopentone in Pediatric Age Group On Cardiovascular SystemDokumen8 halamanComparative Study The Effect of Induction of General Anesthesia With Propofol Versus Thiopentone in Pediatric Age Group On Cardiovascular SystemCentral Asian StudiesBelum ada peringkat
- How To Get TallerDokumen71 halamanHow To Get TallerH0X3M4G1C0% (1)
- BTLDokumen60 halamanBTLCamiBelum ada peringkat
- The Integumentary SystemDokumen11 halamanThe Integumentary SystemHamdy Pagilit DimaporoBelum ada peringkat
- Modul Anatomi Blok 7Dokumen27 halamanModul Anatomi Blok 7Dewandaru I A BBelum ada peringkat
- Overview of Complications Occurring in The Post-Anesthesia Care UnitDokumen14 halamanOverview of Complications Occurring in The Post-Anesthesia Care UnitShahabuddin ShaikhBelum ada peringkat
- Fetal Circulation (For MBBS)Dokumen50 halamanFetal Circulation (For MBBS)Tashif100% (1)
- Brain Basics: John Jefferys and Alison CooperDokumen20 halamanBrain Basics: John Jefferys and Alison CooperswarnBelum ada peringkat
- POLYGRAPHY: THE SCIENTIFIC METHOD OF DETECTING DECEPTIONDokumen15 halamanPOLYGRAPHY: THE SCIENTIFIC METHOD OF DETECTING DECEPTIONEino DuldulaoBelum ada peringkat
- Science: Quarter 1 - Module 1Dokumen10 halamanScience: Quarter 1 - Module 1RUTH PIANGBelum ada peringkat
- 3 9 1 bMSDS-Reagen-LaboratoriumDokumen4 halaman3 9 1 bMSDS-Reagen-Laboratoriumswahyulisah100% (1)
- ICSE Class 10 Biology Previous Year Question Paper 2011 PDFDokumen9 halamanICSE Class 10 Biology Previous Year Question Paper 2011 PDFmohammedBelum ada peringkat
- H2S Training Slides ENGLISHDokumen46 halamanH2S Training Slides ENGLISHf.B100% (1)
- The Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Dokumen10 halamanThe Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Miguel Angel Quiroz CristobalBelum ada peringkat
- Anatomy of A ClamDokumen6 halamanAnatomy of A ClamRU VickBelum ada peringkat
- B CellDokumen10 halamanB CellSonia Elizabeth SimonBelum ada peringkat
- Arthropod-Plant Interactions Novel Insights and Approaches For IPMDokumen238 halamanArthropod-Plant Interactions Novel Insights and Approaches For IPMAnonymous T9uyM2Belum ada peringkat
- Radiation Biology: Presented By: Aarya.H.NairDokumen83 halamanRadiation Biology: Presented By: Aarya.H.NairAARYABelum ada peringkat
- January 2016 (IAL) QP - Unit 1 Edexcel Biology A-LevelDokumen24 halamanJanuary 2016 (IAL) QP - Unit 1 Edexcel Biology A-LevelkirthikaBelum ada peringkat
- Anatomy of The Rat The Nervous SystemDokumen61 halamanAnatomy of The Rat The Nervous SystemBelleopsisBelum ada peringkat
- The Relativistic Brain by Ronald Cicurel and Miguel L. Nicolelis (2015)Dokumen5 halamanThe Relativistic Brain by Ronald Cicurel and Miguel L. Nicolelis (2015)Sinem SerapBelum ada peringkat
- Doppler US Validates Portal Vein Flow in CirrhosisDokumen5 halamanDoppler US Validates Portal Vein Flow in CirrhosisL0v3B00k5Belum ada peringkat
- Meridians and Points PDFDokumen35 halamanMeridians and Points PDFHamdon Hamad100% (9)
- Neurodegenerative Cerebellar AtaxiaDokumen26 halamanNeurodegenerative Cerebellar AtaxiaМилица МилошевићBelum ada peringkat