Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- A Healer S Guide FOr Soul Cleansing - Removing Energies and Entities, Earthbound and ExtraterrestrialDokumen189 halamanA Healer S Guide FOr Soul Cleansing - Removing Energies and Entities, Earthbound and ExtraterrestrialPaulo De Tarso100% (27)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- ABO Blood Group SystemDokumen61 halamanABO Blood Group Systemmail2jackal50% (2)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Clinical Chemistry 2 LectureDokumen46 halamanClinical Chemistry 2 LectureGillian Joy Pagaling100% (1)
- Anxiety DisordersDokumen20 halamanAnxiety DisordersAngela BautistaBelum ada peringkat
- Spermatogenesis PPTDokumen42 halamanSpermatogenesis PPTInsatiable CleeBelum ada peringkat
- Mezoterapija PDFDokumen11 halamanMezoterapija PDFDavid DijakBelum ada peringkat
- Spinal Cord InjuryDokumen97 halamanSpinal Cord Injuryamoon1275% (4)
- M 8 StsDokumen6 halamanM 8 StsGerald Noveda RomanBelum ada peringkat
- Introduction To Bioprocessing and PharmabiotechDokumen34 halamanIntroduction To Bioprocessing and PharmabiotechPeyman SazandehchiBelum ada peringkat
- Virus TableDokumen3 halamanVirus TableFrozenManBelum ada peringkat
- Westie Heal The BookDokumen177 halamanWestie Heal The BookNemo Westie Ogi IIBelum ada peringkat
- Saline or Albumin For Fluid ResuscitationDokumen12 halamanSaline or Albumin For Fluid ResuscitationBill Jones TanawalBelum ada peringkat
- Oral Pregabalin For SEDokumen4 halamanOral Pregabalin For SEBill Jones TanawalBelum ada peringkat
- Progression of Traumatic Intracerebral HemorrhageDokumen15 halamanProgression of Traumatic Intracerebral Hemorrhagegeralders_01Belum ada peringkat
- Refractive Errors and Their Effects On Visual Evoked PotentialsDokumen4 halamanRefractive Errors and Their Effects On Visual Evoked PotentialsBill Jones TanawalBelum ada peringkat
- Herniation and Chronic SDHDokumen5 halamanHerniation and Chronic SDHBill Jones TanawalBelum ada peringkat
- Beginning of LifeDokumen1 halamanBeginning of LifeBill Jones TanawalBelum ada peringkat
- Ischemic Stroke in Young AdultDokumen26 halamanIschemic Stroke in Young AdultBill Jones TanawalBelum ada peringkat
- Burr Holes Tratment in SDH - Gurunathan PDFDokumen4 halamanBurr Holes Tratment in SDH - Gurunathan PDFBill Jones TanawalBelum ada peringkat
- HYPOKALEMIA Periodic ParalysisDokumen15 halamanHYPOKALEMIA Periodic ParalysisBill Jones TanawalBelum ada peringkat
- Novel Approach Selective HypothermiaDokumen1 halamanNovel Approach Selective HypothermiaBill Jones TanawalBelum ada peringkat
- AJRM Sept 18-20 PDFDokumen3 halamanAJRM Sept 18-20 PDFBill Jones TanawalBelum ada peringkat
- Burr Holes Tratment in SDH - Gurunathan PDFDokumen4 halamanBurr Holes Tratment in SDH - Gurunathan PDFBill Jones TanawalBelum ada peringkat
- Hypertensive Retinopathy and Its Association With CVDokumen5 halamanHypertensive Retinopathy and Its Association With CVBill Jones TanawalBelum ada peringkat
- Hypertensive Retinopathy RevisitedDokumen10 halamanHypertensive Retinopathy RevisitedBill Jones TanawalBelum ada peringkat
- Hypertensive Retinopathy and Risk of StrokeDokumen11 halamanHypertensive Retinopathy and Risk of StrokeBill Jones TanawalBelum ada peringkat
- Pulmonary Metastasis of MeningiomaDokumen8 halamanPulmonary Metastasis of MeningiomaBill Jones TanawalBelum ada peringkat
- Anticonvulsant For Preventing Seizures in PX With Chronic SDH - RatilalDokumen11 halamanAnticonvulsant For Preventing Seizures in PX With Chronic SDH - RatilalBill Jones TanawalBelum ada peringkat
- Cerebellar HematomaDokumen13 halamanCerebellar HematomaBill Jones TanawalBelum ada peringkat
- Hypertensive Retinopathy - Eye Disorders - MSD Manual Professional EditionDokumen5 halamanHypertensive Retinopathy - Eye Disorders - MSD Manual Professional EditionBill Jones TanawalBelum ada peringkat
- Images-Hypertensive Retinopathy PDFDokumen7 halamanImages-Hypertensive Retinopathy PDFBill Jones TanawalBelum ada peringkat
- Meningioma Recurrence JournalDokumen15 halamanMeningioma Recurrence JournalBill Jones TanawalBelum ada peringkat
- Syncope Vs Seizure - A Tawakul 07 14 10Dokumen31 halamanSyncope Vs Seizure - A Tawakul 07 14 10Bill Jones TanawalBelum ada peringkat
- Hypertensive RetinopathyDokumen5 halamanHypertensive RetinopathyBill Jones TanawalBelum ada peringkat
- Extraneural Metastasis of Cranial MeningiomaDokumen4 halamanExtraneural Metastasis of Cranial MeningiomaBill Jones TanawalBelum ada peringkat
- Brain Tumors Meningioma Cleaveland ClinicDokumen11 halamanBrain Tumors Meningioma Cleaveland ClinicBill Jones TanawalBelum ada peringkat
- Immediate Recovery of Ischaemic Stroke Following Vitamin b1 AdministrationDokumen2 halamanImmediate Recovery of Ischaemic Stroke Following Vitamin b1 AdministrationBill Jones Tanawal100% (1)
- Brain Tumors Meningioma Cleaveland ClinicDokumen11 halamanBrain Tumors Meningioma Cleaveland ClinicBill Jones TanawalBelum ada peringkat
- Beginning of LifeDokumen1 halamanBeginning of LifeBill Jones TanawalBelum ada peringkat
- MDP10108 Student Guidebook 2023-24-3Dokumen8 halamanMDP10108 Student Guidebook 2023-24-3frinnnaaaaBelum ada peringkat
- 2402 CH 17 Endocrine System (Part 1) PDFDokumen23 halaman2402 CH 17 Endocrine System (Part 1) PDFHarry RussellBelum ada peringkat
- 7 - 5 M Lithium Chloride Precipitation Solution - Unknown - 1832 - UnknownDokumen1 halaman7 - 5 M Lithium Chloride Precipitation Solution - Unknown - 1832 - Unknownmarcos_de_carvalhoBelum ada peringkat
- Human Amyloid Imaging 2015 Book DraftDokumen151 halamanHuman Amyloid Imaging 2015 Book DraftWorldEventsForumBelum ada peringkat
- Colorectal Cancer A ReviewDokumen11 halamanColorectal Cancer A ReviewMarcelitaTaliaDuwiriBelum ada peringkat
- FDA Powerpoint Presentation: Torsades de Pointes and QT ProlongationDokumen51 halamanFDA Powerpoint Presentation: Torsades de Pointes and QT ProlongationByron Harding100% (1)
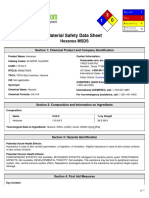
- Msds Heksana - 2 PDFDokumen6 halamanMsds Heksana - 2 PDFrilmaBelum ada peringkat
- 2020-Biochem-Activity-18 - BIOCHEMISTRY OF AGINGDokumen6 halaman2020-Biochem-Activity-18 - BIOCHEMISTRY OF AGINGGabrielle John HernaezBelum ada peringkat
- GeneticsDokumen35 halamanGeneticsSmithBelum ada peringkat
- Human and Animal Physiology Chapter 18 The Central Endocrine GlandsDokumen21 halamanHuman and Animal Physiology Chapter 18 The Central Endocrine Glandshitmanno5Belum ada peringkat
- Mendelian Disorder FinalsDokumen15 halamanMendelian Disorder FinalskanagadurgaBelum ada peringkat
- Innate and Adaptive Immunity: - Innate Is FIRST LINE OF DEFENCE: No Prior Exposure Needed - Comprised OfDokumen31 halamanInnate and Adaptive Immunity: - Innate Is FIRST LINE OF DEFENCE: No Prior Exposure Needed - Comprised OfBegumHazinBelum ada peringkat
- Flores Dorantes 27 Environment and Gene Association With Obesity and Their Impact On Neurodegenerative and Neurodevelopmental DiseasesDokumen24 halamanFlores Dorantes 27 Environment and Gene Association With Obesity and Their Impact On Neurodegenerative and Neurodevelopmental DiseasesPaty BritoBelum ada peringkat
- Lecture On Blood Groups, Transfusion, RH Incompatibility by Dr. RoomiDokumen41 halamanLecture On Blood Groups, Transfusion, RH Incompatibility by Dr. RoomiMudassar Roomi100% (1)
- Medical Test QuestionDokumen2 halamanMedical Test QuestionMohammad TuhinBelum ada peringkat
- 3 CellsDokumen7 halaman3 CellsCaviles, Jasmin S.Belum ada peringkat
- J Child Neurol 2016 Wells 86 92Dokumen7 halamanJ Child Neurol 2016 Wells 86 92Nurul BariyyahBelum ada peringkat
- I.-NCP John Richmond LacadenDokumen3 halamanI.-NCP John Richmond LacadenRichmond Lacaden100% (1)
- tmpB0FF TMPDokumen184 halamantmpB0FF TMPFrontiersBelum ada peringkat
- Human Biology: Unit: 4HB0 Paper: 02Dokumen16 halamanHuman Biology: Unit: 4HB0 Paper: 02Ammatul AyeshaBelum ada peringkat