Anda mungkin juga menyukai
- ACLS Drug TherapyDokumen8 halamanACLS Drug TherapySahrensBelum ada peringkat
- Acls Pharmacology OverviewDokumen11 halamanAcls Pharmacology OverviewzoyaligBelum ada peringkat
- Antiarrhythmic Medication Chart - EBM Consult v3Dokumen2 halamanAntiarrhythmic Medication Chart - EBM Consult v3Linlin100% (1)
- Commonly Used IV Cardiac Medications For Adults Pocket Reference Card PDFDokumen12 halamanCommonly Used IV Cardiac Medications For Adults Pocket Reference Card PDFYannis Zoldenberg100% (1)
- Er FinalsDokumen63 halamanEr FinalsNaren RaviBelum ada peringkat
- Emergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine SulfateDokumen15 halamanEmergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine Sulfate092109Belum ada peringkat
- Overview of Anesthesia - UpToDateDokumen11 halamanOverview of Anesthesia - UpToDateFernandoVianaBelum ada peringkat
- Crisis of Hypertension Revised 1Dokumen57 halamanCrisis of Hypertension Revised 1keenmunir100% (4)
- Emergency Drugs: Cardiac Drugs Atropine SulfateDokumen14 halamanEmergency Drugs: Cardiac Drugs Atropine SulfateJayvee Montoya-Pujante100% (1)
- Anesthesia RecordDokumen1 halamanAnesthesia Recordpcellaneous pc rentalsBelum ada peringkat
- Emergency DrugsDokumen7 halamanEmergency DrugsSara Tongcua TacsagonBelum ada peringkat
- MSK CasesDokumen331 halamanMSK CasesRadio Resident100% (6)
- GambarDokumen27 halamanGambarAnonymous feLB4alTBelum ada peringkat
- IPD - Kardiologi PDFDokumen114 halamanIPD - Kardiologi PDFAnnisa Rahmadhania100% (1)
- M. Pharm Review NAPLEX38Dokumen1 halamanM. Pharm Review NAPLEX38JUSASBBelum ada peringkat
- Adenosine: Rapid IV PushDokumen4 halamanAdenosine: Rapid IV PushsabboBelum ada peringkat
- Pott's Disease NCPDokumen7 halamanPott's Disease NCPkristel_nicole18yahoBelum ada peringkat
- Acute Coronary SyndromeDokumen5 halamanAcute Coronary Syndromem3d1k100% (1)
- Resuscitation Drugs (Ali Haedar)Dokumen41 halamanResuscitation Drugs (Ali Haedar)Bayu AkbarBelum ada peringkat
- Drug Study - TrimetazidineDokumen1 halamanDrug Study - TrimetazidineDanielle Aglusolos50% (2)
- Name of Drug Dose Action Indication Contraindicatio N Side Effect Nurses ResponsibilityDokumen22 halamanName of Drug Dose Action Indication Contraindicatio N Side Effect Nurses ResponsibilityPunam PalBelum ada peringkat
- Obat Obat EmergencyDokumen34 halamanObat Obat EmergencymatkwokBelum ada peringkat
- Peri-Arrest ArrythmiaDokumen14 halamanPeri-Arrest Arrythmiamohamed mowafeyBelum ada peringkat
- Clinical Learning Session-Acute Coronary Syndromes Acs - 1Dokumen31 halamanClinical Learning Session-Acute Coronary Syndromes Acs - 1api-611918048Belum ada peringkat
- Emergency Med ReviewDokumen4 halamanEmergency Med ReviewviaereaBelum ada peringkat
- Obat-Obatan Dalam Bantuan Hidup LanjutDokumen16 halamanObat-Obatan Dalam Bantuan Hidup LanjutTheresia SihotangBelum ada peringkat
- Obat-Obatan ResusitasiDokumen21 halamanObat-Obatan ResusitasiCut Thalya Alissya RahmaBelum ada peringkat
- Cardiac Medications: 1. Antiplatelet Aggregation Therapy: Antiplatelet Aggregation TherapyDokumen14 halamanCardiac Medications: 1. Antiplatelet Aggregation Therapy: Antiplatelet Aggregation TherapyMaria OnofreiBelum ada peringkat
- Dx. StudyDokumen3 halamanDx. Studymayumitanaka8042Belum ada peringkat
- Mi FinalDokumen29 halamanMi Finalmuthu gowthamBelum ada peringkat
- Critical Care Dr. Valerie Zarza GeronDokumen88 halamanCritical Care Dr. Valerie Zarza GeronDivine Grace FernandezBelum ada peringkat
- Hypertensive Urgency EmergencyDokumen5 halamanHypertensive Urgency Emergencydamondouglas100% (3)
- Emergency Medicine: KarsimDokumen39 halamanEmergency Medicine: KarsimNur HikmahBelum ada peringkat
- KEM Protocols - Hypertensive Emergency (Dr. Pritha)Dokumen3 halamanKEM Protocols - Hypertensive Emergency (Dr. Pritha)Sonu AntonyBelum ada peringkat
- CVS1 - K25 - Cardiac EmergencyDokumen34 halamanCVS1 - K25 - Cardiac EmergencyAdmin neuro-usu.idBelum ada peringkat
- Management of Hypertensive EmergencyDokumen35 halamanManagement of Hypertensive EmergencyRaditya Indah TofaniBelum ada peringkat
- Emergency Medicine: KarsimDokumen39 halamanEmergency Medicine: KarsimMuhammad Luqman HakimBelum ada peringkat
- Emd1-K22-Cardiac EmergencyDokumen49 halamanEmd1-K22-Cardiac EmergencyAnanta GintingBelum ada peringkat
- Generic Name: Action: Adverse EffectsDokumen2 halamanGeneric Name: Action: Adverse EffectsSalwa ZeinBelum ada peringkat
- Ventura County Medical Center: Mi Thrombolysis, Management ofDokumen3 halamanVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657Belum ada peringkat
- Management Strategy in Hypertensive Crisis The Role of NicardipineDokumen38 halamanManagement Strategy in Hypertensive Crisis The Role of Nicardipinezulfikar adiBelum ada peringkat
- Tatalaksana ArrthytmiaDokumen55 halamanTatalaksana ArrthytmiaJanstine FirstiandyBelum ada peringkat
- ACLS Algorithms Adult 2010Dokumen12 halamanACLS Algorithms Adult 2010anon_336736395Belum ada peringkat
- IPD - KardiologiDokumen124 halamanIPD - KardiologiAnis BonitaBelum ada peringkat
- Farma StrokeDokumen37 halamanFarma StrokeDAHLIABelum ada peringkat
- Management of MI 2Dokumen24 halamanManagement of MI 2muthu gowthamBelum ada peringkat
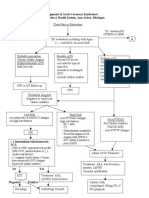
- Management of Acute Coronary Syndromes St. Joseph Mercy Health System, Ann Arbor, MichiganDokumen2 halamanManagement of Acute Coronary Syndromes St. Joseph Mercy Health System, Ann Arbor, MichiganFiorellaBeatrizBelum ada peringkat
- Defibrillate Unsynchronized Cardioversion 200 Joules q2mDokumen3 halamanDefibrillate Unsynchronized Cardioversion 200 Joules q2m[161]Shuaib AktherBelum ada peringkat
- Fármacos CardiacosDokumen2 halamanFármacos CardiacosMARILUZ ROSA NOVOA GUTIERREZBelum ada peringkat
- Stroke Drug Study (GROUP)Dokumen8 halamanStroke Drug Study (GROUP)Fran LanBelum ada peringkat
- Atrial Fibrillation TDDokumen6 halamanAtrial Fibrillation TDapi-594366475Belum ada peringkat
- NSTEMI Management: MHAM-College of MedicineDokumen14 halamanNSTEMI Management: MHAM-College of MedicineMykki Gigi NateBelum ada peringkat
- Tata Laksana Terapi StrokeDokumen18 halamanTata Laksana Terapi StrokeUmmi HabibahBelum ada peringkat
- Drug StudypppDokumen42 halamanDrug Studyppp2022106284Belum ada peringkat
- Algorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSDokumen6 halamanAlgorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSNenyBelum ada peringkat
- ECG SummaryDokumen2 halamanECG SummaryYsabellaPlarisanBelum ada peringkat
- STEMI Thrombolysis Protocol STElevation MIDokumen6 halamanSTEMI Thrombolysis Protocol STElevation MISurya AtmajaBelum ada peringkat
- Registrar Continuing Education: CasesDokumen43 halamanRegistrar Continuing Education: Caseszacks nyirongoBelum ada peringkat
- U.M.F. "Gr. T. Popa" Ia Ş IDokumen37 halamanU.M.F. "Gr. T. Popa" Ia Ş Ij.doe.hex_87Belum ada peringkat
- Emergency Viva (Full)Dokumen48 halamanEmergency Viva (Full)ashokarathnasingheBelum ada peringkat
- PharmaDokumen6 halamanPharmaLovely AmadoBelum ada peringkat
- Syok KardiogenikDokumen31 halamanSyok KardiogenikcantikarevieraBelum ada peringkat
- Unit Farmasi Klinikal (Ufk), Husm.: Atrial Fibrillation in Critical Care - Amiodarone or Digoxin ?Dokumen41 halamanUnit Farmasi Klinikal (Ufk), Husm.: Atrial Fibrillation in Critical Care - Amiodarone or Digoxin ?Ichwan Zuanto SjamanBelum ada peringkat
- Pertemuan 7 LiyanaDokumen36 halamanPertemuan 7 LiyanaLiyana SafitriBelum ada peringkat
- Contoh Tugas Bahasa InggrisDokumen7 halamanContoh Tugas Bahasa InggrisTania ViolantinaBelum ada peringkat
- Comparison of Endoscopic and Surgical Treatment For Acute Cholangitis Caused by CholedocolithiasisDokumen12 halamanComparison of Endoscopic and Surgical Treatment For Acute Cholangitis Caused by CholedocolithiasismonchoellesBelum ada peringkat
- Contoh Research Protocol-V2!18!11 - 05Dokumen11 halamanContoh Research Protocol-V2!18!11 - 05Citra SuciptaBelum ada peringkat
- Role of Presepsin in Determining The Incidence of Septic Shock and Mortality in Patients With SepsisDokumen8 halamanRole of Presepsin in Determining The Incidence of Septic Shock and Mortality in Patients With Sepsisfaraz.mirza1Belum ada peringkat
- Region X: January 1, 2021 Advanced Life Support Standard Operating ProceduresDokumen126 halamanRegion X: January 1, 2021 Advanced Life Support Standard Operating ProceduresC ScribBelum ada peringkat
- Basicinterpretationofcxr 110913060449 Phpapp01Dokumen84 halamanBasicinterpretationofcxr 110913060449 Phpapp01Alexandra DîrțuBelum ada peringkat
- 10 Adult Anesthesia Pre-Operative Evaluation FormDokumen1 halaman10 Adult Anesthesia Pre-Operative Evaluation FormAina HaravataBelum ada peringkat
- Get Vaccinated-Argument EssayDokumen4 halamanGet Vaccinated-Argument Essayapi-489674055Belum ada peringkat
- Spotlight Script Term 2Dokumen11 halamanSpotlight Script Term 2P bmainBelum ada peringkat
- Kerala University of Health Sciences Thrissur: (2010 Scheme)Dokumen1 halamanKerala University of Health Sciences Thrissur: (2010 Scheme)subiBelum ada peringkat
- Suicide: in This ArticleDokumen8 halamanSuicide: in This ArticleDr_Asma86Belum ada peringkat
- Prenatal and Postnatal CareDokumen49 halamanPrenatal and Postnatal CareJOHN ALLEN ALCANTARABelum ada peringkat
- COPD2019Dokumen9 halamanCOPD2019ClintonBelum ada peringkat
- Case Study 5.6.1 JOHNSON AND JOHNSONDokumen2 halamanCase Study 5.6.1 JOHNSON AND JOHNSONnaman0% (1)
- Guideline 133FM PDFDokumen13 halamanGuideline 133FM PDFPangestu DhikaBelum ada peringkat
- Urethral Catheterization 1Dokumen31 halamanUrethral Catheterization 1Hilman HadiansyahBelum ada peringkat
- Under Supervision of Dr. Ommia AliDokumen15 halamanUnder Supervision of Dr. Ommia AliAbdelrhman AboodaBelum ada peringkat
- Peace Corps Vaccine Administration Schedule - TG 300 Medical Technical Guideline 300 - July 2008Dokumen4 halamanPeace Corps Vaccine Administration Schedule - TG 300 Medical Technical Guideline 300 - July 2008Accessible Journal Media: Peace Corps Documents100% (1)
- WHO - Weekly Epidemiological Update On COVID-19 - 22 February 2022Dokumen26 halamanWHO - Weekly Epidemiological Update On COVID-19 - 22 February 2022Adam ForgieBelum ada peringkat
- Shalonda Wright: Professional ExperienceDokumen2 halamanShalonda Wright: Professional Experienceapi-242764074Belum ada peringkat
- Sdm-Mbbs 1st Year-SyllabusDokumen160 halamanSdm-Mbbs 1st Year-SyllabusVinayaka SPBelum ada peringkat
- A.Chn As A Field of Nursing PracticeDokumen1 halamanA.Chn As A Field of Nursing PracticeHanna LopezBelum ada peringkat
- Sean Benesh Resume 10-1-23Dokumen2 halamanSean Benesh Resume 10-1-23api-708800698Belum ada peringkat
- Test Bank For Pathology For The Physical Therapist Assistant 1st Edition by GoodmanDokumen5 halamanTest Bank For Pathology For The Physical Therapist Assistant 1st Edition by Goodmanblanchepandorat6bBelum ada peringkat
- OLHS COVID Phase-IV BackToSchool FlyerDokumen1 halamanOLHS COVID Phase-IV BackToSchool FlyerRachael ThomasBelum ada peringkat