Anda mungkin juga menyukai
- DSM 5 Autism Spectrum Disorder Fact SheetDokumen2 halamanDSM 5 Autism Spectrum Disorder Fact SheetAnonymous Pj6OdjBelum ada peringkat
- HESI Study Guide Psychiatric NursingDokumen26 halamanHESI Study Guide Psychiatric NursingDean Winchester100% (4)
- 2007 MCQDokumen67 halaman2007 MCQTiffani Gutierrez100% (1)
- Use of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFDokumen9 halamanUse of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFJose Luis Granados SolerBelum ada peringkat
- Cars Childhood Autism Rating ScaleDokumen1 halamanCars Childhood Autism Rating ScaleJasudhiar Hu Or Dhiar33% (3)
- Implant Failure and ManagementDokumen59 halamanImplant Failure and ManagementDrIbrahimShaikh0% (1)
- Susan Mathews Case NotesDokumen2 halamanSusan Mathews Case NotesHarshit Aggarwal80% (5)
- Oral Drug Administration: Digracia L. Manatiga RN MAN Chief, Affiliation, NETBDokumen72 halamanOral Drug Administration: Digracia L. Manatiga RN MAN Chief, Affiliation, NETBdigracia manatiga100% (1)
- Dialysis Inspection Tool 2014Dokumen11 halamanDialysis Inspection Tool 2014Maek100% (1)
- Complete Genetics Disease ChartDokumen14 halamanComplete Genetics Disease ChartJames FlanneryBelum ada peringkat
- Ncp-Ineffective Breathing PatternDokumen4 halamanNcp-Ineffective Breathing PatternRoxanne Ganayo Claver100% (1)
- Group 3 Team 1 - Case AnalysisDokumen14 halamanGroup 3 Team 1 - Case AnalysisLaureen CordovaBelum ada peringkat
- Med SurgDokumen3 halamanMed SurgHanako ShigaBelum ada peringkat
- HYDRONEPHROSISDokumen43 halamanHYDRONEPHROSISEureka RathinamBelum ada peringkat
- Doctor's order sheet for Cleopatra AndudeDokumen3 halamanDoctor's order sheet for Cleopatra AndudeRenea Joy ArruejoBelum ada peringkat
- Impaired Gas Exchange NCPDokumen1 halamanImpaired Gas Exchange NCPCj AlconabaBelum ada peringkat
- !the H Book For 5th Year OSCE - Part 1Dokumen147 halaman!the H Book For 5th Year OSCE - Part 1farzzana100% (1)
- Borang Logbook - IndraDokumen15 halamanBorang Logbook - IndraMabokkerupukBelum ada peringkat
- Slide MR 7 - 8 Agustus 2017Dokumen62 halamanSlide MR 7 - 8 Agustus 2017Heru WahyudiBelum ada peringkat
- EMERGENCY REPORT: 9 PATIENTS TREATED FOR INJURIES AND ILLNESSESDokumen96 halamanEMERGENCY REPORT: 9 PATIENTS TREATED FOR INJURIES AND ILLNESSESZakkyMaulanaRahmatBelum ada peringkat
- Laporan Jaga Selasa, 21 Januari 2020Dokumen11 halamanLaporan Jaga Selasa, 21 Januari 2020Amalia SholihahBelum ada peringkat
- 10 September 2019Dokumen20 halaman10 September 2019kumoro panjiBelum ada peringkat
- Emergency Report January 10-11 2017: Chief On Duty: Coass On DutyDokumen83 halamanEmergency Report January 10-11 2017: Chief On Duty: Coass On DutyYulianti Yulianti YuliantiBelum ada peringkat
- Jum'at, 19 Juli 2019 Dokumen Medis Rumah SakitDokumen13 halamanJum'at, 19 Juli 2019 Dokumen Medis Rumah SakitlinggarBelum ada peringkat
- ER 23-24 Juli 2016Dokumen55 halamanER 23-24 Juli 2016Theresia Alfionita SinulinggaBelum ada peringkat
- Morning Report: Rsau Dr. M. Munir Lanud Abd. SalehDokumen10 halamanMorning Report: Rsau Dr. M. Munir Lanud Abd. SalehQonita Prasta AgustiaBelum ada peringkat
- Emergency Abdominal Pain CasesDokumen27 halamanEmergency Abdominal Pain CasesWahyu Hendra PrabowoBelum ada peringkat
- HC SolDokumen30 halamanHC Solmonyet65Belum ada peringkat
- CASE 7: Cerebrovascular Accident, Bleed vs. Infarct: JMJ Marist BrothersDokumen9 halamanCASE 7: Cerebrovascular Accident, Bleed vs. Infarct: JMJ Marist Brothersspain michaelisBelum ada peringkat
- MR 27 Juli 2021Dokumen21 halamanMR 27 Juli 2021kumoro panjiBelum ada peringkat
- Maping Luar Mina Lantai 1, 4 Agustus 2022Dokumen18 halamanMaping Luar Mina Lantai 1, 4 Agustus 2022Fitri DicyBelum ada peringkat
- TIM 1 VISIT SUMMARYDokumen4 halamanTIM 1 VISIT SUMMARYRyan Tantri ArdoBelum ada peringkat
- Emergency: Case ReportDokumen63 halamanEmergency: Case Reporttania jannahBelum ada peringkat
- Divisi Bedah DigestifDokumen6 halamanDivisi Bedah DigestifInkalapheBelum ada peringkat
- MR 24-25 Agustus 2019 FixDokumen67 halamanMR 24-25 Agustus 2019 Fixniah ismaBelum ada peringkat
- 30-Mar-15 Konru NSDokumen3 halaman30-Mar-15 Konru NSAnonymous JXEtV98KjPBelum ada peringkat
- Emergency: Case ReportDokumen63 halamanEmergency: Case Reporttania jannahBelum ada peringkat
- Visite Tim I 23 Sep-1Dokumen3 halamanVisite Tim I 23 Sep-1Frans JobethBelum ada peringkat
- Minggu I (Rsud Abepura) Minggu Ii (Rsud Yowari) Minggu Iii (Anak, BTKV)Dokumen14 halamanMinggu I (Rsud Abepura) Minggu Ii (Rsud Yowari) Minggu Iii (Anak, BTKV)MichelBelum ada peringkat
- Friday, March 3 2023: 1 PatientDokumen15 halamanFriday, March 3 2023: 1 PatientbobbyBelum ada peringkat
- Daftar Pasien RSUP H. Adam Malik MedanDokumen38 halamanDaftar Pasien RSUP H. Adam Malik MedandhinyBelum ada peringkat
- Laporan Jaga Igd: Rsud Adhiyatma, MPH Coass Bedah UnimusDokumen27 halamanLaporan Jaga Igd: Rsud Adhiyatma, MPH Coass Bedah UnimusDony Hamonangan SiregarBelum ada peringkat
- 24 Feb 24 Distribusi Pasien Visite Besar Ilmu Bedah FK ULMDokumen11 halaman24 Feb 24 Distribusi Pasien Visite Besar Ilmu Bedah FK ULMWildan'z CreedBelum ada peringkat
- Emergency Case Report 4 - 5 February 2019: TH THDokumen49 halamanEmergency Case Report 4 - 5 February 2019: TH THmonyet65Belum ada peringkat
- Pomr Dewi 190919Dokumen6 halamanPomr Dewi 190919emjehBelum ada peringkat
- General Census Nov 7Dokumen5 halamanGeneral Census Nov 7Mark Angelo PonferradoBelum ada peringkat
- Daftar Pasien RSUP H. Adam Malik Medan - Senin, 24 Juli 2023Dokumen3 halamanDaftar Pasien RSUP H. Adam Malik Medan - Senin, 24 Juli 2023Admin neuro-usu.idBelum ada peringkat
- EC Epirubicin Cyclophosphamide Adjuvant Neo-Adjuvant Regimen Protocol V1.0Dokumen5 halamanEC Epirubicin Cyclophosphamide Adjuvant Neo-Adjuvant Regimen Protocol V1.0smokkerBelum ada peringkat
- SENSUS BEDAH SARAFDokumen12 halamanSENSUS BEDAH SARAFAbigailGraceBelum ada peringkat
- MappingDokumen4 halamanMappingRina SyafritaBelum ada peringkat
- Laporan Jaga Emergensi Rabu, 29 Mei 2019: Dr. Jaga Pagi - Dr. Jaga Siang - Dr. Jaga MalamDokumen11 halamanLaporan Jaga Emergensi Rabu, 29 Mei 2019: Dr. Jaga Pagi - Dr. Jaga Siang - Dr. Jaga MalamRizky FaisalBelum ada peringkat
- No Identity Admission To E.R. Diagnosis Treatment: Treatment From Brigjen H. Hasan Basry Kandangan HospitalDokumen14 halamanNo Identity Admission To E.R. Diagnosis Treatment: Treatment From Brigjen H. Hasan Basry Kandangan HospitalDewi AngginiBelum ada peringkat
- Emergency Case Report June 8 - 9 2019: TH THDokumen83 halamanEmergency Case Report June 8 - 9 2019: TH THEmma AssagafBelum ada peringkat
- Resume RM 15022023Dokumen1 halamanResume RM 15022023BEDAH UNIVERSITAS ANDALASBelum ada peringkat
- SURGEONS REPORT EMERGENCY ROOM ACTIVITIESDokumen19 halamanSURGEONS REPORT EMERGENCY ROOM ACTIVITIESamal.fathullahBelum ada peringkat
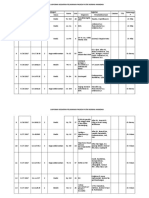
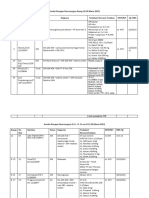
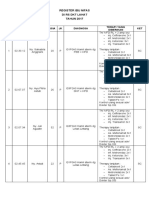
- Register Ibu Nifas 2017Dokumen6 halamanRegister Ibu Nifas 2017jkn rsiampBelum ada peringkat
- Sensus Bangsal Luar 31.10.2022Dokumen7 halamanSensus Bangsal Luar 31.10.2022Gung WistaraBelum ada peringkat
- Emergency: Chief On Duty: Yuli Coass On Duty: Akbar, Febri, FauzanDokumen28 halamanEmergency: Chief On Duty: Yuli Coass On Duty: Akbar, Febri, FauzanahmadfauzanarifaniBelum ada peringkat
- Laporan Jaga Emergensi Senin, 29 April 2019: Dr. Jaga Pagi Dr. Jaga Sore Internship Sore Dr. Jaga MalamDokumen12 halamanLaporan Jaga Emergensi Senin, 29 April 2019: Dr. Jaga Pagi Dr. Jaga Sore Internship Sore Dr. Jaga MalamRizky Faisal Putra SurahmanBelum ada peringkat
- Case 1Dokumen9 halamanCase 1Joselyn M. LachicaBelum ada peringkat
- Update Prime Emergency Unit - MEDIKA 2017Dokumen34 halamanUpdate Prime Emergency Unit - MEDIKA 2017adiborthopaediBelum ada peringkat
- Register Ibu Nifas 2016Dokumen6 halamanRegister Ibu Nifas 2016jkn rsiampBelum ada peringkat
- Finalfinalfinal Medback IeDokumen12 halamanFinalfinalfinal Medback IeBrent SantosBelum ada peringkat
- Don Mariano Marcos Memorial State University Nursing CaseDokumen9 halamanDon Mariano Marcos Memorial State University Nursing CaseJoselyn M. LachicaBelum ada peringkat
- Module 3 - Case 1Dokumen9 halamanModule 3 - Case 1Joselyn M. LachicaBelum ada peringkat
- Morning Report: 1 MARET 2017Dokumen3 halamanMorning Report: 1 MARET 2017samuel jekson kambuayaBelum ada peringkat
- Permohonan Program Kerja MagangDokumen5 halamanPermohonan Program Kerja Magangadrian_benediktusBelum ada peringkat
- Selasa, 30 April 2019: No Identitas Pasien Diagnosis TerapiDokumen11 halamanSelasa, 30 April 2019: No Identitas Pasien Diagnosis TerapiMunadya HamzahBelum ada peringkat
- Aps Sabtu, 17 September 2022Dokumen12 halamanAps Sabtu, 17 September 2022Klinik Praktek Bersama A17Belum ada peringkat
- Date Progress Notes Doctor's Order C AR E DDokumen4 halamanDate Progress Notes Doctor's Order C AR E DRenea Joy ArruejoBelum ada peringkat
- Laporan Jaga Emergensi Senin, 21 Mei 2018: Dr. Jaga Pagi Dr. Jaga Sore Dr. Jaga MalemDokumen68 halamanLaporan Jaga Emergensi Senin, 21 Mei 2018: Dr. Jaga Pagi Dr. Jaga Sore Dr. Jaga MalemBayu EwanggaBelum ada peringkat
- Pasien Igd Bedah Kamis, 5 April 2018 Dr. Jaga: Nut/ Leo/ Bro/ Bay/ Sel/ Tom No. CM Nama Umur/JK Diagnosa Utama Tindakan Jam Masuk MRS/ Pulang KetDokumen1 halamanPasien Igd Bedah Kamis, 5 April 2018 Dr. Jaga: Nut/ Leo/ Bro/ Bay/ Sel/ Tom No. CM Nama Umur/JK Diagnosa Utama Tindakan Jam Masuk MRS/ Pulang Kettrifamonika23Belum ada peringkat
- Aflp, Ka, RV, byDokumen22 halamanAflp, Ka, RV, byNatasha AnditaBelum ada peringkat
- 14-11-22 Malam Dr. YolaDokumen6 halaman14-11-22 Malam Dr. YolabobynandaBelum ada peringkat
- Atlas of Parathyroid Imaging and PathologyDari EverandAtlas of Parathyroid Imaging and PathologyAlexander L. ShifrinBelum ada peringkat
- Imunisasi Tetanus Dan Difteri Untuk RemajaDokumen4 halamanImunisasi Tetanus Dan Difteri Untuk RemajaRully SyahrizalBelum ada peringkat
- DAFTAR PUSTAKA RevisiDokumen2 halamanDAFTAR PUSTAKA RevisiRully SyahrizalBelum ada peringkat
- LAPORAN PAGI ANESTESI OPERASI CITO JAM DINASDokumen1 halamanLAPORAN PAGI ANESTESI OPERASI CITO JAM DINASRully SyahrizalBelum ada peringkat
- Practice Advisory For Preanesthesia EvaluationDokumen17 halamanPractice Advisory For Preanesthesia EvaluationAdrian WirahamediBelum ada peringkat
- Bab IDokumen2 halamanBab IRully SyahrizalBelum ada peringkat
- Lumbar Laminectomy Diskectomy Fusion PDFDokumen3 halamanLumbar Laminectomy Diskectomy Fusion PDFRully SyahrizalBelum ada peringkat
- Emergency Room Morning Report: October 16th 2017Dokumen68 halamanEmergency Room Morning Report: October 16th 2017Rully SyahrizalBelum ada peringkat
- Bab IiDokumen18 halamanBab IiRully SyahrizalBelum ada peringkat
- Emergency Room Morning Report: October 16th 2017Dokumen68 halamanEmergency Room Morning Report: October 16th 2017Rully SyahrizalBelum ada peringkat
- Jurnal PenelitianDokumen1 halamanJurnal PenelitianRully SyahrizalBelum ada peringkat
- A Pocket Guide To Blood Pressure Measurement in ChildrenDokumen4 halamanA Pocket Guide To Blood Pressure Measurement in ChildrenKira23406Belum ada peringkat
- WHO 2016 Brain Tumor ClassificationDokumen18 halamanWHO 2016 Brain Tumor ClassificationMu ZBelum ada peringkat
- Journal Reading: "Direct Current Stimulation of The Ear in Tinnitus Treatment: A Double-Blind Placebo-Controlled Study"Dokumen16 halamanJournal Reading: "Direct Current Stimulation of The Ear in Tinnitus Treatment: A Double-Blind Placebo-Controlled Study"Rully SyahrizalBelum ada peringkat
- Journal Reading: "Direct Current Stimulation of The Ear in Tinnitus Treatment: A Double-Blind Placebo-Controlled Study"Dokumen16 halamanJournal Reading: "Direct Current Stimulation of The Ear in Tinnitus Treatment: A Double-Blind Placebo-Controlled Study"Rully SyahrizalBelum ada peringkat
- Mrs. Afiah /29 TH MRS Tgl. 23-03-2017 Pkl. 22:15 WITA SubjectiveDokumen5 halamanMrs. Afiah /29 TH MRS Tgl. 23-03-2017 Pkl. 22:15 WITA SubjectiveRully SyahrizalBelum ada peringkat
- Emergency C-Section for Breech Presentation with Cord ProlapseDokumen7 halamanEmergency C-Section for Breech Presentation with Cord ProlapseRully SyahrizalBelum ada peringkat
- Cairan Dan Shock KoasDokumen31 halamanCairan Dan Shock KoasRully SyahrizalBelum ada peringkat
- Mapping Tulip 2B (Bangsal Cempaka) : Ny. Nurhayati/ 40 / Kista Ovarium Curiga GanasDokumen1 halamanMapping Tulip 2B (Bangsal Cempaka) : Ny. Nurhayati/ 40 / Kista Ovarium Curiga GanasRully SyahrizalBelum ada peringkat
- Mounsey & McCarthy - Curr Op - 2013Dokumen8 halamanMounsey & McCarthy - Curr Op - 2013Rully SyahrizalBelum ada peringkat
- LGM LGM D 09 1Dokumen7 halamanLGM LGM D 09 1Rully SyahrizalBelum ada peringkat
- IASP Wait TimesDokumen5 halamanIASP Wait TimesalexandruBelum ada peringkat
- Blood Pressure Variability: How To Deal?: NR Rau, Gurukanth RaoDokumen5 halamanBlood Pressure Variability: How To Deal?: NR Rau, Gurukanth RaoRully SyahrizalBelum ada peringkat
- Mounsey & McCarthy - Curr Op - 2013Dokumen8 halamanMounsey & McCarthy - Curr Op - 2013Rully SyahrizalBelum ada peringkat
- Facit-Ai Eng Final Ver4 20nov08Dokumen1 halamanFacit-Ai Eng Final Ver4 20nov08Rully SyahrizalBelum ada peringkat
- 14 DSM5 Systematic Review and MetaanalysisDokumen15 halaman14 DSM5 Systematic Review and MetaanalysisRully SyahrizalBelum ada peringkat
- Lisa ManningDokumen10 halamanLisa ManningRully SyahrizalBelum ada peringkat
- BPV LengkapDokumen13 halamanBPV LengkapRully SyahrizalBelum ada peringkat
- Ebp Picc Line - RevisedDokumen6 halamanEbp Picc Line - Revisedapi-234544335Belum ada peringkat
- Sodium Chromate Anhydrous PDFDokumen6 halamanSodium Chromate Anhydrous PDFErika WidiariniBelum ada peringkat
- Nutrition of Aging DogsDokumen19 halamanNutrition of Aging DogsBrisbany AlcibarBelum ada peringkat
- A Tertiary Health Care Centre Experience of The Impact of COVID On The Case Load in The Department of Obstetrics and Gynaecology at MGM Hospital, AurangabadDokumen4 halamanA Tertiary Health Care Centre Experience of The Impact of COVID On The Case Load in The Department of Obstetrics and Gynaecology at MGM Hospital, AurangabadInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Antimicrobial Activity of Disinfectants Commonly Used in The Food Industry in MexicoDokumen6 halamanAntimicrobial Activity of Disinfectants Commonly Used in The Food Industry in MexicoJoel CarinoBelum ada peringkat
- Bailey 5th Ed. 2014 (1125-1318) - TraumaDokumen194 halamanBailey 5th Ed. 2014 (1125-1318) - TraumaelFadhlyBelum ada peringkat
- Application of Recombinant DNADokumen2 halamanApplication of Recombinant DNANathan B. MhineBelum ada peringkat
- FNDRC Vol 2 AppendicesDokumen43 halamanFNDRC Vol 2 AppendicesJohn Michael Macabenta100% (1)
- For The Best Sinus Congestion RemediesDokumen4 halamanFor The Best Sinus Congestion Remedies4zaleakuBelum ada peringkat
- Risk Prediction Model for Heart Failure in DiabetesDokumen20 halamanRisk Prediction Model for Heart Failure in DiabetesjamesboendBelum ada peringkat
- Substance AbuseDokumen16 halamanSubstance AbuseAkansha JohnBelum ada peringkat
- Studies On The Stability of Chicken IgY in Different Sugars Complex Carbohydrates and Food MaterialsDokumen12 halamanStudies On The Stability of Chicken IgY in Different Sugars Complex Carbohydrates and Food MaterialsJohnrel SecretariaBelum ada peringkat
- The Paleopathology of Specific Infectious Diseases From Southeastern Hungary: A Brief OverviewDokumen6 halamanThe Paleopathology of Specific Infectious Diseases From Southeastern Hungary: A Brief OverviewLucía Chavarría RíosBelum ada peringkat
- Maternity Clinical Network Contact DetailsDokumen18 halamanMaternity Clinical Network Contact DetailsAlina-Gabriela MarinBelum ada peringkat
- Carbetocin For The Prevention of Postpartum HemorrhageDokumen8 halamanCarbetocin For The Prevention of Postpartum HemorrhageLeslie GuzmanBelum ada peringkat
- Afeccion Ocular y Blefaroconjuntivitis Por Leishmania de HumanosDokumen4 halamanAfeccion Ocular y Blefaroconjuntivitis Por Leishmania de HumanosPilar Sanchez GuiraoBelum ada peringkat
- TB PosterDokumen1 halamanTB PosterSucie 1997Belum ada peringkat