Anda mungkin juga menyukai
- Clinical - Pharmacokinetics 3rd Year BushDokumen53 halamanClinical - Pharmacokinetics 3rd Year BushBaguma MichaelBelum ada peringkat
- Pharmacology (Dr. Nico)Dokumen41 halamanPharmacology (Dr. Nico)stella pangestikaBelum ada peringkat
- PkineticsDokumen8 halamanPkineticsmlbranham2753Belum ada peringkat
- 9 Mô hình hai ngăn, Không tuyến tính, PKPDDokumen45 halaman9 Mô hình hai ngăn, Không tuyến tính, PKPDthuong nguyen thiBelum ada peringkat
- Pharmacokinetics: Drug Absorption, Distribution, Metabolism and ExcretionDokumen55 halamanPharmacokinetics: Drug Absorption, Distribution, Metabolism and ExcretionLs Tamil editzzBelum ada peringkat
- Basic & Clinical PKDokumen24 halamanBasic & Clinical PKGopal pokhrelBelum ada peringkat
- Absorption, Distribution, Metabolism and Excretion: Prof. Ian Hughes, 9.83, I.e.hughes@leeds - Ac.ukDokumen41 halamanAbsorption, Distribution, Metabolism and Excretion: Prof. Ian Hughes, 9.83, I.e.hughes@leeds - Ac.uksaisunnyram100% (1)
- Eneral Pharmacology: PharmacokineticsDokumen36 halamanEneral Pharmacology: PharmacokineticsSupreet Singh MalhiBelum ada peringkat
- Pharmacokinetics overviewDokumen21 halamanPharmacokinetics overviewPh SamerBelum ada peringkat
- Principles of Toxicokinetics and ToxicodynamicsDokumen70 halamanPrinciples of Toxicokinetics and Toxicodynamicskiki rawitriBelum ada peringkat
- FarmakokinetikaDokumen142 halamanFarmakokinetikaAstrid Bernadette Ulina PurbaBelum ada peringkat
- 10bioavailability AbsorptionDokumen67 halaman10bioavailability AbsorptionNikki ChauhanBelum ada peringkat
- Pharmacokinetics PDFDokumen78 halamanPharmacokinetics PDFKate EvangelistaBelum ada peringkat
- Clinical PharmacokineticsDokumen39 halamanClinical PharmacokineticsParijatBelum ada peringkat
- Pharmacokinetics SPLE June 2021Dokumen55 halamanPharmacokinetics SPLE June 2021Syeda Ayesha FarhanaBelum ada peringkat
- Excretion and Elimination KineticsDokumen39 halamanExcretion and Elimination KineticsYashasv BhatnagarBelum ada peringkat
- Drug-body interactions PK and PD overviewDokumen45 halamanDrug-body interactions PK and PD overviewWalaa abo foolBelum ada peringkat
- CVVH Vs CVVHDDokumen26 halamanCVVH Vs CVVHDMasoud Es'haghiniaBelum ada peringkat
- Principle of Drug Action 2021Dokumen31 halamanPrinciple of Drug Action 2021cindy8127Belum ada peringkat
- Non Linear PharmacokineticsDokumen64 halamanNon Linear PharmacokineticsMoganaa LakshmiBelum ada peringkat
- Nonlinear PharmacokineticsDokumen28 halamanNonlinear PharmacokineticsPrashant PandeyBelum ada peringkat
- Basic pharmacokinetics and its clinical applicationsDokumen43 halamanBasic pharmacokinetics and its clinical applicationsPhilippe KinnaerBelum ada peringkat
- Anesthesia Drugs Part 1 and 2 CompiledDokumen20 halamanAnesthesia Drugs Part 1 and 2 CompiledLavBelum ada peringkat
- Absorption of DrugsDokumen34 halamanAbsorption of Drugsalexpharm100% (1)
- Pharmacokinetic ModelsDokumen36 halamanPharmacokinetic ModelsNeeraj Kumar100% (1)
- Pharmacokinetics & Pharmacodynamics of Controlled Release SystemsDokumen33 halamanPharmacokinetics & Pharmacodynamics of Controlled Release SystemsSumant SainiBelum ada peringkat
- Pharmacokinetics & Pharmacodynamics ExplainedDokumen2 halamanPharmacokinetics & Pharmacodynamics Explainedgeldevera100% (1)
- UNDERSTANDING FIRST-PASS METABOLISM AND BIOAVAILABILITYDokumen37 halamanUNDERSTANDING FIRST-PASS METABOLISM AND BIOAVAILABILITYFitrye Yhana Rayyi KurniawanBelum ada peringkat
- Clinical Pharmacokinetics and Pharmacodynamics: Dr. Abaasi KabogoDokumen52 halamanClinical Pharmacokinetics and Pharmacodynamics: Dr. Abaasi KabogoNina100% (1)
- Drug Absorption: Dr. Chandane R. DDokumen54 halamanDrug Absorption: Dr. Chandane R. DBandameedi RamuBelum ada peringkat
- Pharmacokinetics PHDokumen71 halamanPharmacokinetics PHCasper ScholesBelum ada peringkat
- 6 PharmacokineticsDokumen7 halaman6 PharmacokineticsMd Sakil AminBelum ada peringkat
- Principles of Drug ActionDokumen42 halamanPrinciples of Drug ActionsharmamtechBelum ada peringkat
- المعلومات بالداخل موثوق بها لنها مراجعه و معتمده من Certified from Pharmacists_coffee magazineDokumen20 halamanالمعلومات بالداخل موثوق بها لنها مراجعه و معتمده من Certified from Pharmacists_coffee magazineMedhat EyadaBelum ada peringkat
- Clinical Pharmacokinetics: Time Course of Drug in the BodyDokumen121 halamanClinical Pharmacokinetics: Time Course of Drug in the BodySuryaAtmajayaBelum ada peringkat
- Physiology Body FluidsDokumen41 halamanPhysiology Body FluidsMalikIrfanAasiBelum ada peringkat
- Clin PK 1-4Dokumen105 halamanClin PK 1-4Klye SahagunBelum ada peringkat
- 3.Ch 11&13desired Plasma Concentration and Volume of DistributionDokumen37 halaman3.Ch 11&13desired Plasma Concentration and Volume of DistributionshougBelum ada peringkat
- 1.1.1 Pharmacokinetics 2022 - 2023Dokumen65 halaman1.1.1 Pharmacokinetics 2022 - 2023brightgyan082Belum ada peringkat
- Clinical - PharmacokineticsDokumen39 halamanClinical - PharmacokineticsSreya SanilBelum ada peringkat
- Nonlinear Pharmacokinetics: Guided By: Dhaivat C. ParikhDokumen46 halamanNonlinear Pharmacokinetics: Guided By: Dhaivat C. ParikhTushar Bambharoliya100% (5)
- Pharmacology Viva Manual Prefinal PDFDokumen112 halamanPharmacology Viva Manual Prefinal PDF9821699080100% (1)
- General PharmacologyDokumen13 halamanGeneral Pharmacologymalkalhmaidh03Belum ada peringkat
- (Crespy 2002) Quercetin, But Not Its Glycosides, Is Absorbed Fromthe Rat StomachDokumen4 halaman(Crespy 2002) Quercetin, But Not Its Glycosides, Is Absorbed Fromthe Rat StomachSie ningsihBelum ada peringkat
- MHallworth Therapeutic Drug MonitoringDokumen58 halamanMHallworth Therapeutic Drug Monitoringmonday125Belum ada peringkat
- Pharmacokinetic of Simvastatin Study in Malaysian SubjectsDokumen6 halamanPharmacokinetic of Simvastatin Study in Malaysian SubjectsNur Ilham SaputraBelum ada peringkat
- Pharmacokinetics: Bioavailability Volume of Distribution (VD)Dokumen2 halamanPharmacokinetics: Bioavailability Volume of Distribution (VD)Ibraheem SairiBelum ada peringkat
- Toxicokinetics: "What The Body Does To The Toxic Material"Dokumen44 halamanToxicokinetics: "What The Body Does To The Toxic Material"Muhammad Shahid BilalBelum ada peringkat
- Trepanier2013 Applying Pharmacokinetics To Veterinary Clinical PracticeDokumen14 halamanTrepanier2013 Applying Pharmacokinetics To Veterinary Clinical PracticeSarahBelum ada peringkat
- Renal TOLO - Week 3Dokumen6 halamanRenal TOLO - Week 3CarolineJiaBelum ada peringkat
- PharmacokineticsDokumen7 halamanPharmacokineticsJan KarnowskiBelum ada peringkat
- @OCOM IV InfusionDokumen19 halaman@OCOM IV InfusionRAVINDRA BABUBelum ada peringkat
- Pharmacokinetic Principles of Chemical DispositionDokumen59 halamanPharmacokinetic Principles of Chemical DispositionsadwikaBelum ada peringkat
- Drug ClearanceDokumen18 halamanDrug ClearanceMeenahil ZaibBelum ada peringkat
- Pharmacokinetics and Pharmacodynamics in The Critically Ill ChildDokumen21 halamanPharmacokinetics and Pharmacodynamics in The Critically Ill ChildLobo CarterBelum ada peringkat
- Pharmacokinetics - DrdhritiDokumen83 halamanPharmacokinetics - Drdhritidbrahma100% (1)
- 2Dokumen4 halaman2ani bandasoBelum ada peringkat
- Weekly Report Bagian BSDokumen22 halamanWeekly Report Bagian BSani bandasoBelum ada peringkat
- 2Dokumen4 halaman2ani bandasoBelum ada peringkat
- Weekly Report Bagian UrologiDokumen25 halamanWeekly Report Bagian Urologiani bandasoBelum ada peringkat
- Immune Response To Mycobacteral Infection (Copy)Dokumen23 halamanImmune Response To Mycobacteral Infection (Copy)ani bandasoBelum ada peringkat
- Hepatotoxic Drugs: Direct, Indirect and Immune Reaction TypesDokumen17 halamanHepatotoxic Drugs: Direct, Indirect and Immune Reaction Typesani bandasoBelum ada peringkat
- Tadulako Inf. in Children RevDokumen63 halamanTadulako Inf. in Children Revani bandasoBelum ada peringkat
- Fungal and Parasitic Infection in DermatologyDokumen37 halamanFungal and Parasitic Infection in Dermatologyani bandasoBelum ada peringkat
- Hepatotoxic Drugs: Direct, Indirect and Immune Reaction TypesDokumen17 halamanHepatotoxic Drugs: Direct, Indirect and Immune Reaction Typesani bandasoBelum ada peringkat
- Fraktur Humerus Referat Hanum PDFDokumen74 halamanFraktur Humerus Referat Hanum PDFani bandasoBelum ada peringkat
- Pediatric Pneumonia: Signs, Diagnosis and TreatmentDokumen29 halamanPediatric Pneumonia: Signs, Diagnosis and TreatmentNur NurhasyanahBelum ada peringkat
- Tadulako Inf. in Children RevDokumen63 halamanTadulako Inf. in Children Revani bandasoBelum ada peringkat
- Dr. Mei Neni, Adaptation and Physiology of The NewbornDokumen39 halamanDr. Mei Neni, Adaptation and Physiology of The Newbornani bandasoBelum ada peringkat
- Childhood Nephrotic Syndrome-tadulakoApril2014Dokumen28 halamanChildhood Nephrotic Syndrome-tadulakoApril2014ani bandasoBelum ada peringkat
- Dr. Mei Neni, Deteksi Dini Gangguan PerkembanganDokumen43 halamanDr. Mei Neni, Deteksi Dini Gangguan Perkembanganani bandasoBelum ada peringkat
- 6 TorchDokumen64 halaman6 Torchani bandasoBelum ada peringkat
- Hepatitis & It's ComplicationDokumen11 halamanHepatitis & It's ComplicationHadjar Mingfan FlamerBelum ada peringkat
- Dr. Growth and Development of AdolescenceDokumen39 halamanDr. Growth and Development of Adolescenceani bandasoBelum ada peringkat
- UTI Childhood Tadulako2015Dokumen38 halamanUTI Childhood Tadulako2015ani bandasoBelum ada peringkat
- Pediatric Pneumonia: Signs, Diagnosis and TreatmentDokumen29 halamanPediatric Pneumonia: Signs, Diagnosis and TreatmentNur NurhasyanahBelum ada peringkat
- Tadulako Inf in Neonate RevDokumen71 halamanTadulako Inf in Neonate Revani bandasoBelum ada peringkat
- Chronic DiarrheaDokumen7 halamanChronic Diarrheaani bandasoBelum ada peringkat
- Acute Heart Failure: Venice Chairiadi, MD, FIHADokumen55 halamanAcute Heart Failure: Venice Chairiadi, MD, FIHANdz1Belum ada peringkat
- Allergy Diseases in Children: Sumadiono Pediatric Department Faculty of Medicine Gadjah Mada University YogyakartaDokumen43 halamanAllergy Diseases in Children: Sumadiono Pediatric Department Faculty of Medicine Gadjah Mada University Yogyakartaani bandasoBelum ada peringkat
- Abnormal Urinalysis Children-Tadulako2015Dokumen33 halamanAbnormal Urinalysis Children-Tadulako2015ani bandasoBelum ada peringkat
- UTI Childhood Tadulako2015Dokumen38 halamanUTI Childhood Tadulako2015ani bandasoBelum ada peringkat
- Abnormal Urinalysis Children-Tadulako2015Dokumen33 halamanAbnormal Urinalysis Children-Tadulako2015ani bandasoBelum ada peringkat
- HypertensionDokumen51 halamanHypertensionani bandasoBelum ada peringkat
- Valvular Heaart DiseaseDokumen38 halamanValvular Heaart Diseaseani bandasoBelum ada peringkat
- 14 Anterolateral Thigh FlapDokumen6 halaman14 Anterolateral Thigh FlapAngga Putra100% (1)
- AnaesthesiaDokumen5 halamanAnaesthesiaAnonymous 4jkFIRalKBelum ada peringkat
- Rajah 1 Di Bawah Menunjukkan Struktur Sejenis Sel.: Bahagian A (20 Markah)Dokumen12 halamanRajah 1 Di Bawah Menunjukkan Struktur Sejenis Sel.: Bahagian A (20 Markah)maysaraBelum ada peringkat
- Synevo Results 5Dokumen3 halamanSynevo Results 5Kenan BagirBelum ada peringkat
- Snaprevise Biology A2 Revision CheatsheetDokumen15 halamanSnaprevise Biology A2 Revision CheatsheetSomaya AliBelum ada peringkat
- Dental and anesthesia procedures and equipmentDokumen56 halamanDental and anesthesia procedures and equipmentVijay RanaBelum ada peringkat
- Biology Savemyexam NotesDokumen4 halamanBiology Savemyexam NotesSayeef MahdiBelum ada peringkat
- AVA ASA Hi ElectronicDokumen2 halamanAVA ASA Hi ElectronicJonathan ZapataBelum ada peringkat
- The History and Pathology of CrucifixionDokumen4 halamanThe History and Pathology of Crucifixiondondinax_182746269Belum ada peringkat
- GyyggDokumen11 halamanGyyggYaumil AqsaBelum ada peringkat
- 282-Essentials of Pain Management-Nalini Vadivelu Richard D. Urman Roberta L. Hines-0387875786-Sp PDFDokumen859 halaman282-Essentials of Pain Management-Nalini Vadivelu Richard D. Urman Roberta L. Hines-0387875786-Sp PDFarief-024100% (2)
- Farmakologi Antiagina TTMDokumen83 halamanFarmakologi Antiagina TTMEpha Lumban GaolBelum ada peringkat
- Encyclopedia of Gastroenterology PDFDokumen2.352 halamanEncyclopedia of Gastroenterology PDFAndor Claudia Florentina100% (1)
- LP Surgery ChestDokumen6 halamanLP Surgery Chestangelmd83Belum ada peringkat
- Lab Report - Smooth MuscleDokumen8 halamanLab Report - Smooth MuscledhebbertBelum ada peringkat
- Pelod ScoreDokumen7 halamanPelod ScoreAgus SarjonoBelum ada peringkat
- IsopreneDokumen5 halamanIsopreneArdynaApriSapoetriBelum ada peringkat
- The Acute NeurologiDokumen343 halamanThe Acute Neurologizee zeeBelum ada peringkat
- How to Dilute Blood and Count White Blood CellsDokumen2 halamanHow to Dilute Blood and Count White Blood CellsAlfred ChowBelum ada peringkat
- How Your Diet Affects Your BrainDokumen2 halamanHow Your Diet Affects Your BrainRusso Dalmasso50% (2)
- Fundamentals of Respiratory Sounds and AnalysisDokumen68 halamanFundamentals of Respiratory Sounds and AnalysisVaidotas NorkūnasBelum ada peringkat
- Animal KingdomDokumen30 halamanAnimal KingdomRupa MitraBelum ada peringkat
- Human Brain: Presented by Ayesha KhanDokumen20 halamanHuman Brain: Presented by Ayesha KhanDilshad JanBelum ada peringkat
- Men in BrainsDokumen9 halamanMen in BrainshenryhempsteadBelum ada peringkat
- Patrick Ch19 p2Dokumen31 halamanPatrick Ch19 p2NizarAliBelum ada peringkat
- Comparison Between Intrauterine Insemination With Ovulation Induction Versus Natural Ovulatory Cycle in Male Factor of InfertilityDokumen74 halamanComparison Between Intrauterine Insemination With Ovulation Induction Versus Natural Ovulatory Cycle in Male Factor of InfertilityMohammed Ahmed AzabBelum ada peringkat
- KIT CD117 A Review On Expression in Normal and Neoplastic TissuesDokumen16 halamanKIT CD117 A Review On Expression in Normal and Neoplastic TissuesVlado VladBelum ada peringkat
- 5 SenseDokumen27 halaman5 Sensechici azriniBelum ada peringkat
- Exam Questions Aqa Trilogy Bioenergetics: Q1-6 Foundaton Q3-9 HigherDokumen28 halamanExam Questions Aqa Trilogy Bioenergetics: Q1-6 Foundaton Q3-9 Higherapi-422428700Belum ada peringkat
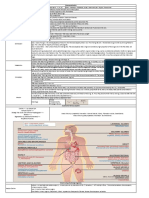
- Human Anatomy and Physiology Study Guide 1Dokumen12 halamanHuman Anatomy and Physiology Study Guide 1api-637418753Belum ada peringkat