Anda mungkin juga menyukai
- NEET PG 2013 Rank List of Eligible CandidatesDokumen256 halamanNEET PG 2013 Rank List of Eligible CandidatesBruno75% (8)
- Hospital Policy ManualDokumen26 halamanHospital Policy ManualBasant GuptaBelum ada peringkat
- Kenya Health Policy 2014 2030Dokumen87 halamanKenya Health Policy 2014 2030Migori ArtBelum ada peringkat
- DR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsDokumen32 halamanDR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsBruno100% (1)
- Prehospital Trauma Care PDFDokumen827 halamanPrehospital Trauma Care PDFAdriana VickBelum ada peringkat
- Bullying in Residency Training ArticleDokumen10 halamanBullying in Residency Training ArticleFiryal BalushiBelum ada peringkat
- Supracondylar Fractures: Bui Thi Huong Group 6-Y3B Saint Paul HospitalDokumen24 halamanSupracondylar Fractures: Bui Thi Huong Group 6-Y3B Saint Paul HospitalHườngBelum ada peringkat
- 22ca ColonDokumen21 halaman22ca ColonDrVishal BhattBelum ada peringkat
- Proceedings of The National Workshop On INTRODUCING YOGA IN MEDICAL CURRICULUMDokumen76 halamanProceedings of The National Workshop On INTRODUCING YOGA IN MEDICAL CURRICULUMYogacharya Dr Ananda Balayogi Bhavanani0% (1)
- Fracture Femur: Presented By: Erin Triana Ronald TejoprayitnoDokumen29 halamanFracture Femur: Presented By: Erin Triana Ronald Tejoprayitnoronald_tejopray742Belum ada peringkat
- Human Organ Tranplantation ActDokumen6 halamanHuman Organ Tranplantation ActFrank NobodBelum ada peringkat
- Buccal CancerDokumen30 halamanBuccal CancerPriscilla ChantalBelum ada peringkat
- Basic Infection Prevention and Control For Hospital Staff and Healthcare ProvidersDokumen60 halamanBasic Infection Prevention and Control For Hospital Staff and Healthcare ProvidersaringkinkingBelum ada peringkat
- Virtual SurgeryDokumen22 halamanVirtual SurgeryMounika Surapaneni100% (1)
- EMS Burn Management PDFDokumen30 halamanEMS Burn Management PDFRaymond Sitanaja0% (1)
- Discuss The Pathogenesis and Management of Periprosthetic Joint InfectionDokumen30 halamanDiscuss The Pathogenesis and Management of Periprosthetic Joint InfectionNURA MUHAMMAD ALIYUBelum ada peringkat
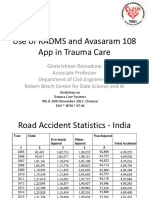
- Prof Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryDokumen37 halamanProf Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryBrunoBelum ada peringkat
- CA ColonDokumen47 halamanCA ColonrahayuBelum ada peringkat
- Skin Grafting SurgeryDokumen15 halamanSkin Grafting SurgeryVithikaBelum ada peringkat
- Operating Room Attire 2018Dokumen5 halamanOperating Room Attire 2018andrea rabangBelum ada peringkat
- Surgery, General, Wounds and Wound HealingDokumen15 halamanSurgery, General, Wounds and Wound HealingRhazes78100% (1)
- Panel DiscussionDokumen5 halamanPanel DiscussionArpit MehraBelum ada peringkat
- Bites and Stings PPT Fix DR IsyaDokumen61 halamanBites and Stings PPT Fix DR IsyamadeBelum ada peringkat
- Periprosthetic Infection: Farry, DRDokumen15 halamanPeriprosthetic Infection: Farry, DRFarry DoankBelum ada peringkat
- Surgical TermsDokumen10 halamanSurgical TermsCLaui SagibalBelum ada peringkat
- Rheumatoid ArthritisDokumen19 halamanRheumatoid ArthritisElvisBelum ada peringkat
- Day Care SurgeryDokumen5 halamanDay Care SurgeryazharmoBelum ada peringkat
- Approach To Fracture BoneDokumen46 halamanApproach To Fracture BoneMuhaimin Noor AzharBelum ada peringkat
- Guidelines For Management of Head InjuryDokumen18 halamanGuidelines For Management of Head InjuryChellamani UmakanthanBelum ada peringkat
- Hepatocellular Carcinoma: Dr. Isbandiyah, SPPDDokumen26 halamanHepatocellular Carcinoma: Dr. Isbandiyah, SPPDMeta ShofiaBelum ada peringkat
- Medical Health Examination FormDokumen4 halamanMedical Health Examination FormAldwin Bagtas0% (1)
- Principles of Trauma ManagementDokumen60 halamanPrinciples of Trauma ManagementDrArish Mahmood100% (1)
- Intestinal Tuberculosis Recent AdvancesDokumen80 halamanIntestinal Tuberculosis Recent AdvancesVijay KumarBelum ada peringkat
- Day Case Surgery 1LDokumen21 halamanDay Case Surgery 1LdrhiwaomerBelum ada peringkat
- Legal Medicine CasesDokumen139 halamanLegal Medicine Casesmuton20Belum ada peringkat
- PT in Integumentary ConditionsDokumen16 halamanPT in Integumentary ConditionsJiggs Lim0% (1)
- Tumor Markers Dr. MarwaDokumen36 halamanTumor Markers Dr. Marwakholoud220Belum ada peringkat
- Congenital Corneal DisordersDokumen101 halamanCongenital Corneal Disorderseyemd_in_training100% (1)
- Facial InjuriesDokumen61 halamanFacial InjuriesafifrspmBelum ada peringkat
- OMCDokumen37 halamanOMCyurie_ameliaBelum ada peringkat
- Organ Donation Act of 1991Dokumen10 halamanOrgan Donation Act of 1991Dayledaniel Sorveto100% (1)
- Case Report Supracondylar Fracture of Right FemurDokumen37 halamanCase Report Supracondylar Fracture of Right FemurSri Mahtufa Riski100% (1)
- Medico-Legal Aspect of Physical Injuries: Dr. Rowena M. Cuevillas ProfessorDokumen127 halamanMedico-Legal Aspect of Physical Injuries: Dr. Rowena M. Cuevillas ProfessorAccu Xii VhenzBelum ada peringkat
- Squamous Cell CarcinomaDokumen18 halamanSquamous Cell CarcinomaNurul Izzah Mat SundariBelum ada peringkat
- Chimerism Definition, Symptoms, Testing, Diagnosis, and MoreDokumen1 halamanChimerism Definition, Symptoms, Testing, Diagnosis, and MoreWunmi LateefBelum ada peringkat
- Malunion Delayed Union and Nonunion FracturesDokumen31 halamanMalunion Delayed Union and Nonunion Fracturessatya yudhayanaBelum ada peringkat
- 100 Medical TerminologiesDokumen4 halaman100 Medical TerminologiesCzarina Mae Quinones TadeoBelum ada peringkat
- 4 H Surgical Instruments and TerminologyDokumen17 halaman4 H Surgical Instruments and TerminologyMahmoud Hussien100% (1)
- Lectures in Forensic MedicineDokumen3 halamanLectures in Forensic MedicinelindagabitBelum ada peringkat
- Lecture Notes On Surgery - Part II - Dr. Yogiram BolisettyDokumen79 halamanLecture Notes On Surgery - Part II - Dr. Yogiram Bolisettyjun sianBelum ada peringkat
- Gynecological Instruments: Surgical Instruments Images & NamesDokumen4 halamanGynecological Instruments: Surgical Instruments Images & NamesGenevang SeaweedsBelum ada peringkat
- Hospital Disclosure PolicyDokumen10 halamanHospital Disclosure Policyvks7876Belum ada peringkat
- Preoperative ChecklistDokumen3 halamanPreoperative Checklistraj1969Belum ada peringkat
- GDL 2010-04-14 SET Recruitment Booklet V9Dokumen23 halamanGDL 2010-04-14 SET Recruitment Booklet V9juweriy100% (1)
- 2ndary Malignant Tumor BoneDokumen2 halaman2ndary Malignant Tumor Bonetahir_the_great2939Belum ada peringkat
- Conservative Treatment of Diaphyseal Fractures of Tibia andDokumen40 halamanConservative Treatment of Diaphyseal Fractures of Tibia andsaihaBelum ada peringkat
- DVT & PeDokumen57 halamanDVT & PeRashed ShatnawiBelum ada peringkat
- Crush Injury of Hand PDFDokumen22 halamanCrush Injury of Hand PDFmilananand0% (1)
- (POLI TRAUMA) Decision Making in Trauma SurgeryDokumen15 halaman(POLI TRAUMA) Decision Making in Trauma SurgeryEdward Ojeda100% (1)
- Head Injury: Tsegazeab Laeke, MD, FCS (ECSA) August 1,2018Dokumen38 halamanHead Injury: Tsegazeab Laeke, MD, FCS (ECSA) August 1,2018Amanuel AyladoBelum ada peringkat
- Surgical Ethics: Maj. HafizDokumen10 halamanSurgical Ethics: Maj. HafizHafizur Rashid100% (1)
- Types of WoundsDokumen2 halamanTypes of WoundsMike Luther ManingoBelum ada peringkat
- Chapter 01 PDFDokumen14 halamanChapter 01 PDFMeera KrishnanBelum ada peringkat
- Comprehensive Healthcare Simulation: Mobile Medical SimulationDari EverandComprehensive Healthcare Simulation: Mobile Medical SimulationPatricia K. CarstensBelum ada peringkat
- Prof - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenDokumen40 halamanProf - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenBrunoBelum ada peringkat
- Hub and Spoke Model For STEMI Management - Tamil Nadu ModelDokumen16 halamanHub and Spoke Model For STEMI Management - Tamil Nadu ModelBrunoBelum ada peringkat
- Prof DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesDokumen42 halamanProf DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesBrunoBelum ada peringkat
- DR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonDokumen25 halamanDR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonBrunoBelum ada peringkat
- DR - Ramana Rao Pre-Hospital Services in Tamil NaduDokumen73 halamanDR - Ramana Rao Pre-Hospital Services in Tamil NaduBrunoBelum ada peringkat
- TAEI NTRI WorkshopDokumen16 halamanTAEI NTRI WorkshopBrunoBelum ada peringkat
- Ms Ellaine Boo Role of Trauma NursingDokumen35 halamanMs Ellaine Boo Role of Trauma NursingBrunoBelum ada peringkat
- Prof Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryDokumen37 halamanProf Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryBrunoBelum ada peringkat
- DR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianDokumen36 halamanDR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianBruno100% (1)
- Doctors' Role in Tackling Organ TradeDokumen70 halamanDoctors' Role in Tackling Organ TradeBrunoBelum ada peringkat
- Prof DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsDokumen36 halamanProf DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsBrunoBelum ada peringkat
- Prof Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareDokumen21 halamanProf Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareBrunoBelum ada peringkat
- DR - Darez Ahamed Vision For Tamil NaduDokumen6 halamanDR - Darez Ahamed Vision For Tamil NaduBrunoBelum ada peringkat
- Mr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusDokumen25 halamanMr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusBruno100% (1)
- DR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemDokumen29 halamanDR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemBrunoBelum ada peringkat
- Neurology, Neurosurgery MCQ PointsDokumen32 halamanNeurology, Neurosurgery MCQ PointsBruno86% (7)
- HMIS - Health Management Information System - Government of Tamil NaduDokumen12 halamanHMIS - Health Management Information System - Government of Tamil NaduBruno100% (1)
- TN Gazette 47 of 2013 Part VI Section 4Dokumen84 halamanTN Gazette 47 of 2013 Part VI Section 4BrunoBelum ada peringkat
- MRB Detailed Notification 31032013Dokumen7 halamanMRB Detailed Notification 31032013BrunoBelum ada peringkat
- GO5509 ResidenDokumen4 halamanGO5509 ResidenBrunoBelum ada peringkat
- Go (MS) 329Dokumen1 halamanGo (MS) 329BrunoBelum ada peringkat
- Go (MS) 533Dokumen7 halamanGo (MS) 533BrunoBelum ada peringkat
- Illustration 1: Pay Band 4Dokumen4 halamanIllustration 1: Pay Band 4BrunoBelum ada peringkat
- Go (MS) 519Dokumen1 halamanGo (MS) 519BrunoBelum ada peringkat
- Ccs Postings DetailDokumen5 halamanCcs Postings DetailBrunoBelum ada peringkat
- 1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingDokumen14 halaman1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingKamx Mohammed100% (1)
- PP-2525 EMS Radio Report Format PDFDokumen2 halamanPP-2525 EMS Radio Report Format PDFNunuy NuriahBelum ada peringkat
- Narrative Report For ER and PSODokumen2 halamanNarrative Report For ER and PSOIshay FerrerBelum ada peringkat
- Alex Alas MSN, Agcns: 6285 Andersen Mills Heights - 336-837-7183Dokumen3 halamanAlex Alas MSN, Agcns: 6285 Andersen Mills Heights - 336-837-7183api-700587394Belum ada peringkat
- Emergency NursingDokumen5 halamanEmergency NursingmirageplayerBelum ada peringkat
- ED Volunteer ManualDokumen15 halamanED Volunteer Manualkape1oneBelum ada peringkat
- Nursing ResumeDokumen2 halamanNursing Resumeapi-259457383Belum ada peringkat
- Director &HOD Prof - Dr. K.PRAKASAM M.S.Ortho, D.Ortho, DSC (Hon)Dokumen70 halamanDirector &HOD Prof - Dr. K.PRAKASAM M.S.Ortho, D.Ortho, DSC (Hon)vimalBelum ada peringkat
- Covid-19 Contingency Plan PDFDokumen27 halamanCovid-19 Contingency Plan PDFRodgelyn FranciscoBelum ada peringkat
- Bug Defect Triage ProcessDokumen20 halamanBug Defect Triage Processraulnq50% (2)
- Triase 1Dokumen8 halamanTriase 1Anonymous GpgioaDAbBelum ada peringkat
- Unit 7 Trauma and Triage: Kelompok 5: Agus Widayanti Mika Apriyanti Yudi Yuda SaputraDokumen17 halamanUnit 7 Trauma and Triage: Kelompok 5: Agus Widayanti Mika Apriyanti Yudi Yuda SaputraZulkarnainBelum ada peringkat
- TRIAGEDokumen55 halamanTRIAGELaveena AswaleBelum ada peringkat
- ER NurseDokumen3 halamanER NurseDhanNie CenitaBelum ada peringkat
- Short Term Training Curriculum Handbook - EMT-B - 1 June 2017 - 1Dokumen48 halamanShort Term Training Curriculum Handbook - EMT-B - 1 June 2017 - 1navneetBelum ada peringkat
- Jade Abbott - Mls Hidden TasksDokumen78 halamanJade Abbott - Mls Hidden TasksMudit JainBelum ada peringkat
- Principles and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Dokumen17 halamanPrinciples and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Sae TumBelum ada peringkat
- En Notes EscDokumen7 halamanEn Notes EscCG Patron BamboBelum ada peringkat
- Trauma TriageDokumen24 halamanTrauma TriageImam AdiBelum ada peringkat
- PlaningDokumen86 halamanPlaningStephen MendezBelum ada peringkat
- Disaster Nursing: Norman G. CalderonDokumen79 halamanDisaster Nursing: Norman G. Calderonelaine_reodica100% (1)
- Health Assessment Phemap 2009Dokumen67 halamanHealth Assessment Phemap 2009SergeGaudielBelum ada peringkat
- Emp09 PDFDokumen5 halamanEmp09 PDFKarthik SBelum ada peringkat
- Using A Theory To Understand Triage Decision MakingDokumen5 halamanUsing A Theory To Understand Triage Decision MakingwilmaBelum ada peringkat
- Emergency Protocol ProcedureDokumen14 halamanEmergency Protocol Procedurejmmos207064Belum ada peringkat
- Medical Surgical Nursing Lecture I MonthlyDokumen9 halamanMedical Surgical Nursing Lecture I MonthlyJohn Lyndon SayongBelum ada peringkat
- TTDokumen200 halamanTTaneem khanBelum ada peringkat
- SGBV SopDokumen72 halamanSGBV SopMigori ArtBelum ada peringkat