Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Aha SVTDokumen69 halamanAha SVTdeardiarymysteryBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Nasi Lemak Restaurants in Bangsar VillageDokumen1 halamanNasi Lemak Restaurants in Bangsar VillageAndy XiaoBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Case 3 CA Nasofaring Dr. Oscar, SPTHTDokumen16 halamanCase 3 CA Nasofaring Dr. Oscar, SPTHTAndy XiaoBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Aorta: Normal Radiological Reference ValuesDokumen3 halamanAorta: Normal Radiological Reference ValuesJha K SujitBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Who FCH Cah 06.1Dokumen123 halamanWho FCH Cah 06.1Ðr SalmaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Case OMA DR - Oscar, SPTHTDokumen29 halamanCase OMA DR - Oscar, SPTHTAndy XiaoBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Who FCH Cah 06.1Dokumen123 halamanWho FCH Cah 06.1Ðr SalmaBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Water Imaging FetusDokumen9 halamanWater Imaging FetusAndy XiaoBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Referat Farmakologi Obat AnestesiDokumen11 halamanReferat Farmakologi Obat AnestesiAndy XiaoBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- NASOPHARYNGEAL CARCINOMA CASE PRESENTATIONDokumen37 halamanNASOPHARYNGEAL CARCINOMA CASE PRESENTATIONAndy XiaoBelum ada peringkat
- Anatomy of The Ear FixDokumen40 halamanAnatomy of The Ear FixAndy XiaoBelum ada peringkat
- CJC 31 04 185Dokumen12 halamanCJC 31 04 185Azan Al RasyidBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Angina Ludovici EmergenciesDokumen5 halamanAngina Ludovici EmergenciesAndy XiaoBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Laboratory: Anne Z - Saunders, Andrea Vallen Stein, and Nancy Lite ShusterDokumen3 halamanLaboratory: Anne Z - Saunders, Andrea Vallen Stein, and Nancy Lite ShusterAndy XiaoBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Poster 10 NLS 01 01 ENG V20100927 PDFDokumen1 halamanPoster 10 NLS 01 01 ENG V20100927 PDFAndy XiaoBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Poster 10 NLS 01 01 ENG V20100927 PDFDokumen1 halamanPoster 10 NLS 01 01 ENG V20100927 PDFAndy XiaoBelum ada peringkat
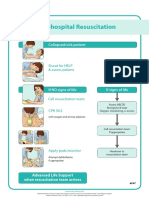
- Poster 10 IHBLS 01 01 ENG V20100927Dokumen1 halamanPoster 10 IHBLS 01 01 ENG V20100927Andy XiaoBelum ada peringkat
- Poster 10 PALS 01 01 ENG V20100927 PDFDokumen1 halamanPoster 10 PALS 01 01 ENG V20100927 PDFAndy XiaoBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Basic Life Support & Automated External Defibrillation: Check ResponseDokumen1 halamanBasic Life Support & Automated External Defibrillation: Check ResponseAndy XiaoBelum ada peringkat
- Poster 10 ALS-TACH 01 01 ENG V20100927Dokumen1 halamanPoster 10 ALS-TACH 01 01 ENG V20100927Andy XiaoBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Iv 133Dokumen4 halamanIv 133Andy XiaoBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Poster 10 ALS-BRAD 01 01 ENG V20100927Dokumen1 halamanPoster 10 ALS-BRAD 01 01 ENG V20100927Andy XiaoBelum ada peringkat
- Iv 111Dokumen11 halamanIv 111Andy XiaoBelum ada peringkat
- Universal Algorithm: Advanced Life SupportDokumen1 halamanUniversal Algorithm: Advanced Life SupportAndy XiaoBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- 10.1 Life-Threatening Electrolyte AbnormalitiesDokumen6 halaman10.1 Life-Threatening Electrolyte AbnormalitiesWidya WidyariniBelum ada peringkat
- Cardioversion, and Pacing Part 5: Electrical Therapies: Automated External Defibrillators, DefibrillationDokumen13 halamanCardioversion, and Pacing Part 5: Electrical Therapies: Automated External Defibrillators, DefibrillationAndy XiaoBelum ada peringkat
- Iv 136Dokumen4 halamanIv 136Andy XiaoBelum ada peringkat
- Iv 89Dokumen23 halamanIv 89Andy XiaoBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Iv 84 PDFDokumen6 halamanIv 84 PDFAndy XiaoBelum ada peringkat
- An Intergenerational Approach to Family TherapyDokumen31 halamanAn Intergenerational Approach to Family TherapyBeatriz Eugenia Guerra100% (5)
- Chapter 1Dokumen15 halamanChapter 1ErikaBelum ada peringkat
- DCTMDDokumen58 halamanDCTMDHanzara PanolBelum ada peringkat
- Closed Tibia and Fibula Fracture Case PresentationDokumen30 halamanClosed Tibia and Fibula Fracture Case Presentationzhafran_darwisBelum ada peringkat
- BLEEDING TIME AND CLOTTING TIME TESTSDokumen30 halamanBLEEDING TIME AND CLOTTING TIME TESTScharutha gopalBelum ada peringkat
- Post Partum ExamDokumen4 halamanPost Partum ExamAhby Vitug de Luna100% (1)
- Vivekananda Kendra NRL HospitalDokumen29 halamanVivekananda Kendra NRL HospitalVivekananda Kendra100% (1)
- CLASS 1 - Image - Roles Revised June 260Dokumen48 halamanCLASS 1 - Image - Roles Revised June 260Marie-Lynne L'orBelum ada peringkat
- Youtsey Kristen Cover LetterDokumen1 halamanYoutsey Kristen Cover Letterapi-457850399Belum ada peringkat
- Food and Exercise LogDokumen24 halamanFood and Exercise LogmhetfieldBelum ada peringkat
- Nurture and ConnectionDokumen4 halamanNurture and Connectionparents021100% (1)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- DUR - Fracture of The Shaft Radius and UlnaDokumen55 halamanDUR - Fracture of The Shaft Radius and UlnaM. Abdurrahman Al-HaraaniBelum ada peringkat
- Route of Administration PDFDokumen45 halamanRoute of Administration PDFBurhan MubasharBelum ada peringkat
- Closing The Gap 2012Dokumen127 halamanClosing The Gap 2012ABC News OnlineBelum ada peringkat
- 1 s2.0 S0022391302002998 MainDokumen5 halaman1 s2.0 S0022391302002998 MainManjeev GuragainBelum ada peringkat
- ColostomyDokumen5 halamanColostomyZhyraine Iraj D. Caluza100% (1)
- Nexthealth - Semantic Web Sparks Evolution of Health 2.0 - A Road Map To Consumer-Centric HealthcareDokumen7 halamanNexthealth - Semantic Web Sparks Evolution of Health 2.0 - A Road Map To Consumer-Centric HealthcareMaarten den Braber100% (43)
- Create Consent Form (39 charactersDokumen3 halamanCreate Consent Form (39 charactersJan Diel100% (2)
- Juvenile Sex Offenders A Complex PopulationDokumen6 halamanJuvenile Sex Offenders A Complex PopulationRoberto GalleguillosBelum ada peringkat
- Supine Cervical Traction After Anterior Cervical Diskectomy and FusionDokumen4 halamanSupine Cervical Traction After Anterior Cervical Diskectomy and FusionOscar NgBelum ada peringkat
- Fatal Airway Obstruction Due To Ludwig'sDokumen6 halamanFatal Airway Obstruction Due To Ludwig'sRegina MugopalBelum ada peringkat
- Introduction To Dental Anatomy: DR - Yad Raouf BDS, Efb, MrcsedDokumen27 halamanIntroduction To Dental Anatomy: DR - Yad Raouf BDS, Efb, MrcsedRabarBelum ada peringkat
- Water Sealed DrainageDokumen2 halamanWater Sealed DrainagefairwoodsBelum ada peringkat
- Adr FormDokumen2 halamanAdr FormSachin Kumar PrajapatiBelum ada peringkat
- Demand and ElasticityDokumen5 halamanDemand and ElasticityCorey Crismon100% (1)
- Compartment SyndromeDokumen29 halamanCompartment SyndromeFazmial UjirBelum ada peringkat
- CV Sef Disciplina Victor Lorin PurcareaDokumen8 halamanCV Sef Disciplina Victor Lorin PurcareaMircea LeonardBelum ada peringkat
- Indian Journal of Applied Basic Medical Science Sept - 2008Dokumen28 halamanIndian Journal of Applied Basic Medical Science Sept - 2008soham2007Belum ada peringkat
- Gallbladder and Bile Duct Anatomy, Function and DiseasesDokumen16 halamanGallbladder and Bile Duct Anatomy, Function and DiseasesKadenceFreya-Charisse G PosadasBulintao100% (2)
- Klasifikasi Penyebab KomaDokumen19 halamanKlasifikasi Penyebab KomaNoni JacksonBelum ada peringkat