Anda mungkin juga menyukai
- Perioperative NursingDokumen74 halamanPerioperative NursingTina Talmadge100% (4)
- Job Description of A Nurse AnesthetistDokumen3 halamanJob Description of A Nurse AnesthetistlhalamBelum ada peringkat
- Medication Adherence Questionnaire (MAQ) : ARMS ScaleDokumen4 halamanMedication Adherence Questionnaire (MAQ) : ARMS ScaleEnesaHodžićBelum ada peringkat
- Fall Risk Assessment FormDokumen3 halamanFall Risk Assessment FormMichael Silva100% (1)
- Carlin Smith Child Abuse FinalDokumen12 halamanCarlin Smith Child Abuse FinalCarlin SmithBelum ada peringkat
- Family Case AnalysisDokumen194 halamanFamily Case AnalysisDianneBelum ada peringkat
- PACU Discharge CriteriaDokumen1 halamanPACU Discharge CriteriaTarquin Tomada100% (2)
- Recovery Room Transfer SheetDokumen1 halamanRecovery Room Transfer SheetDr. Sumit Kumbhar0% (1)
- Onset Positions in Induction of Anesthesia Spinal Anesthesia Nitrous Oxide Respiratory Complications Respiratory ObstructionDokumen7 halamanOnset Positions in Induction of Anesthesia Spinal Anesthesia Nitrous Oxide Respiratory Complications Respiratory ObstructionArvin Ian Penaflor50% (2)
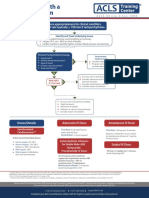
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDokumen1 halamanAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahBelum ada peringkat
- Ed Assessment Tool SampleDokumen28 halamanEd Assessment Tool SampleAnonymous ibmeej9Belum ada peringkat
- Admitting A Patient .: Prepared by Ayugi Winnyfred Patience Bsc. Midwifery StudentDokumen10 halamanAdmitting A Patient .: Prepared by Ayugi Winnyfred Patience Bsc. Midwifery StudentAYO NELSONBelum ada peringkat
- Upload 8Dokumen2 halamanUpload 8cingyaBelum ada peringkat
- Ipcr Kabisote Ob orDokumen2 halamanIpcr Kabisote Ob orAr JayBelum ada peringkat
- Drug Study Paracetamol Ambroxol Ascorbic Acid CefuroximeDokumen5 halamanDrug Study Paracetamol Ambroxol Ascorbic Acid CefuroximeCia TriiBelum ada peringkat
- Intensive Care UnitDokumen12 halamanIntensive Care UnitAnt OnBelum ada peringkat
- Responsibilites of A PACU NurseDokumen1 halamanResponsibilites of A PACU NurseTarquin TomadaBelum ada peringkat
- Pressure Ulcer Prevention and Managment PolicyDokumen32 halamanPressure Ulcer Prevention and Managment PolicybudimanBelum ada peringkat
- Or ConceptsDokumen70 halamanOr ConceptsArnulfo ArmamentoBelum ada peringkat
- Nursing Care of Post Anesthesia Patients OutlinedDokumen13 halamanNursing Care of Post Anesthesia Patients OutlinedRhea JessicaBelum ada peringkat
- Emergency NursingDokumen15 halamanEmergency NursingAshley Ishika100% (1)
- CCUDokumen82 halamanCCUSarah100% (1)
- Annex I Summary of Product CharacteristicsDokumen28 halamanAnnex I Summary of Product CharacteristicsEmma SinBelum ada peringkat
- Procedure Manual HospitalDokumen196 halamanProcedure Manual HospitalMarian StrihaBelum ada peringkat
- Emergency Department Operational SOP v1.1 Mar2017Dokumen15 halamanEmergency Department Operational SOP v1.1 Mar2017agelesswapBelum ada peringkat
- Vital SignsDokumen51 halamanVital SignsEstelita M. Dela CruzBelum ada peringkat
- Ic-01-041 Infection Control in DialysisDokumen15 halamanIc-01-041 Infection Control in DialysisDerick RanaBelum ada peringkat
- Management of The EVDDokumen7 halamanManagement of The EVDplethoraldork100% (1)
- Blood Transfusion Single Use PathwayDokumen6 halamanBlood Transfusion Single Use PathwayropusanBelum ada peringkat
- Cardiovascular FunctionDokumen157 halamanCardiovascular FunctionJonnabelle PadillaBelum ada peringkat
- Continuous Quality Improvement IndicatorsDokumen10 halamanContinuous Quality Improvement Indicatorsaaminah tariq100% (1)
- Medical Triage Codes ExplainedDokumen3 halamanMedical Triage Codes ExplainedAnieaj Buj LevineBelum ada peringkat
- Sree Vasantham Hospital, Salem: 1. Er Protocol For Acute Intoxication (Poisoning)Dokumen7 halamanSree Vasantham Hospital, Salem: 1. Er Protocol For Acute Intoxication (Poisoning)Elango MuthuBelum ada peringkat
- Trauma NurseDokumen11 halamanTrauma Nurseapi-247119922Belum ada peringkat
- Bsn-Rs-Careplan 2Dokumen9 halamanBsn-Rs-Careplan 2api-520841770Belum ada peringkat
- Code Blue System: Hospital Sultanah Aminah Johor BahruDokumen15 halamanCode Blue System: Hospital Sultanah Aminah Johor BahrumursidahanimBelum ada peringkat
- Acute Respiratory Distress: Section I: Scenario DemographicsDokumen6 halamanAcute Respiratory Distress: Section I: Scenario DemographicsharasthaBelum ada peringkat
- Blood Transfusions - TGH Policies & ProceduresDokumen4 halamanBlood Transfusions - TGH Policies & ProceduresMark Anthony FranciscoBelum ada peringkat
- 4e Ospital NG SampalocDokumen113 halaman4e Ospital NG SampalocJomar RicablancaBelum ada peringkat
- Operating Room Nurse Interview QuestionsDokumen2 halamanOperating Room Nurse Interview Questionsali aliBelum ada peringkat
- Emergency Nursing: By: Keverne Jhay P. ColasDokumen61 halamanEmergency Nursing: By: Keverne Jhay P. ColasGaras AnnaBerniceBelum ada peringkat
- Welcome TO Intensive Care UnitDokumen42 halamanWelcome TO Intensive Care UnitKharene Lirazan100% (1)
- BASIC LIFE SUPPORT: ESSENTIAL CONCEPTS AND PROCEDURESDokumen8 halamanBASIC LIFE SUPPORT: ESSENTIAL CONCEPTS AND PROCEDURESHynne Jhea EchavezBelum ada peringkat
- Triage PDFDokumen59 halamanTriage PDFagungBelum ada peringkat
- PRE ANAESTHETIC ASSESSMENT New 1Dokumen41 halamanPRE ANAESTHETIC ASSESSMENT New 1lokeswara reddyBelum ada peringkat
- 3.preoperative Patient Assessment and ManagementDokumen76 halaman3.preoperative Patient Assessment and Managementoliyad alemayehuBelum ada peringkat
- Assessment Algorithm For Sedated Adult ICU Patients: No YesDokumen18 halamanAssessment Algorithm For Sedated Adult ICU Patients: No YeshendraBelum ada peringkat
- AbbreviationDokumen19 halamanAbbreviationJayson NatividadBelum ada peringkat
- Emergency NursingDokumen46 halamanEmergency NursingJoshua P AloveroBelum ada peringkat
- Supine Hypotensive Syndrome Signs, Causes and TreatmentDokumen6 halamanSupine Hypotensive Syndrome Signs, Causes and TreatmentDimas RadityaBelum ada peringkat
- Nursing BulletsDokumen83 halamanNursing BulletsgilissaBelum ada peringkat
- Assigned on Admission, Transfer, and Discharge ProceduresDokumen12 halamanAssigned on Admission, Transfer, and Discharge ProceduresNagulan Nagul100% (1)
- The Triage ProcessDokumen3 halamanThe Triage ProcessepingBelum ada peringkat
- Informed Consent 1Dokumen11 halamanInformed Consent 1Edah HumaidahBelum ada peringkat
- Self Assessment ToolkitDokumen43 halamanSelf Assessment Toolkitshah007zaad100% (1)
- Anxiolytic and Hypnotic AgentsDokumen50 halamanAnxiolytic and Hypnotic AgentsMoxie Macado100% (1)
- Recovery Room NurseDokumen5 halamanRecovery Room NurseChristin 'Kirei' AndoloBelum ada peringkat
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDari EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsBelum ada peringkat
- NURSING CARE OF ADULTS II: Passbooks Study GuideDari EverandNURSING CARE OF ADULTS II: Passbooks Study GuideBelum ada peringkat
- Status EpilepticusDokumen14 halamanStatus EpilepticusAhmad Shafwan NatsirBelum ada peringkat
- Difficult AirwayDokumen22 halamanDifficult AirwayLamtioma GultomBelum ada peringkat
- Gangguan Saraf Tepi Dr. Yetti PrintDokumen41 halamanGangguan Saraf Tepi Dr. Yetti PrintLamtioma GultomBelum ada peringkat
- Journal Reading Airway Management and Smoke Inhalation Injury in The Burn PatientDokumen36 halamanJournal Reading Airway Management and Smoke Inhalation Injury in The Burn PatientMiftahuljannah SudirmanBelum ada peringkat
- Treatment of Scabies: Comparative Study of EfficacyDokumen7 halamanTreatment of Scabies: Comparative Study of EfficacyLamtioma GultomBelum ada peringkat
- Hipoksemia in COPDDokumen10 halamanHipoksemia in COPDAnonymous SMLzNABelum ada peringkat
- Treatment of Scabies: Comparative Study of EfficacyDokumen7 halamanTreatment of Scabies: Comparative Study of EfficacyLamtioma GultomBelum ada peringkat
- Class 7 PolityDokumen10 halamanClass 7 PolityNakka nikithaBelum ada peringkat
- Healy Professional DeviceDokumen1 halamanHealy Professional DeviceBramarish KadakuntlaBelum ada peringkat
- Sysman Safety-Integrated-5ed en PDFDokumen345 halamanSysman Safety-Integrated-5ed en PDFErdincBelum ada peringkat
- Thesis-Android-Based Health-Care Management System: July 2016Dokumen66 halamanThesis-Android-Based Health-Care Management System: July 2016Noor Md GolamBelum ada peringkat
- ASP ProductsDokumen33 halamanASP ProductsSerghei Barba100% (1)
- Journal Club Presentation: DR Waleed AhmadDokumen30 halamanJournal Club Presentation: DR Waleed Ahmadkaram aliBelum ada peringkat
- Laboratory Hygiene and SafetyDokumen34 halamanLaboratory Hygiene and SafetyResmiBelum ada peringkat
- UV-VIS Method for Estimating Fat-Soluble Vitamins in MultivitaminsDokumen6 halamanUV-VIS Method for Estimating Fat-Soluble Vitamins in MultivitaminsTisenda TimiselaBelum ada peringkat
- Clinical Biomechanics in Implant DentistryDokumen36 halamanClinical Biomechanics in Implant DentistryMahadevan Ravichandran100% (4)
- Biology 3rd ESO Full DossierDokumen54 halamanBiology 3rd ESO Full DossierNinaBelum ada peringkat
- S.P.P.M. MasterDokumen126 halamanS.P.P.M. MasterwahyuBelum ada peringkat
- Paul B. Bishop, DC, MD, PHD, Jeffrey A. Quon, DC, PHD, FCCSC, Charles G. Fisher, MD, MHSC, FRCSC, Marcel F.S. Dvorak, MD, FRCSCDokumen10 halamanPaul B. Bishop, DC, MD, PHD, Jeffrey A. Quon, DC, PHD, FCCSC, Charles G. Fisher, MD, MHSC, FRCSC, Marcel F.S. Dvorak, MD, FRCSCorlando moraBelum ada peringkat
- Jacked at Home - Bodyweight Muscle-Building WorkoutsDokumen6 halamanJacked at Home - Bodyweight Muscle-Building Workoutsmohamed aliBelum ada peringkat
- Per. Dev. (Bin-Bin)Dokumen21 halamanPer. Dev. (Bin-Bin)Jayric BanagyoBelum ada peringkat
- Common Assessment Framework FormDokumen9 halamanCommon Assessment Framework FormparaypanBelum ada peringkat
- Pta ResumeDokumen2 halamanPta Resumeapi-669470996Belum ada peringkat
- Methodology Tapping Methodology of WaterlineDokumen15 halamanMethodology Tapping Methodology of WaterlineBryBelum ada peringkat
- hdf492 Portfolio PresentationDokumen14 halamanhdf492 Portfolio Presentationapi-403412647Belum ada peringkat
- Stress Amongst Healthcare Professionals and Migrant Workers During Covid-19 PandemicDokumen6 halamanStress Amongst Healthcare Professionals and Migrant Workers During Covid-19 PandemicIJAR JOURNALBelum ada peringkat
- Ethics in Practice - at End of Life - Part 1Dokumen20 halamanEthics in Practice - at End of Life - Part 1anushavergheseBelum ada peringkat
- Manu SkripDokumen20 halamanManu SkripzanimarBelum ada peringkat
- Ergonomics (Uu Tien Dich)Dokumen6 halamanErgonomics (Uu Tien Dich)Phong D LeBelum ada peringkat
- MANAGEMENT AND PREVENTIONDokumen6 halamanMANAGEMENT AND PREVENTIONIrina BalutaBelum ada peringkat
- Human Sexual Response Physiology PhasesDokumen2 halamanHuman Sexual Response Physiology PhasesLovely HerreraBelum ada peringkat
- Hahnemann Advance MethodDokumen2 halamanHahnemann Advance MethodRehan AnisBelum ada peringkat
- Newborn Care Volume 1 2020-1Dokumen192 halamanNewborn Care Volume 1 2020-1Shyvonne PeirisBelum ada peringkat
- 3D Printing Technology in Drug Delivery: Recent Progress and ApplicationDokumen10 halaman3D Printing Technology in Drug Delivery: Recent Progress and ApplicationAngela DelarmenteBelum ada peringkat