Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Nursing Council CXC Past Paper MCQ (1) (319) IMPORTANTDokumen25 halamanNursing Council CXC Past Paper MCQ (1) (319) IMPORTANTAaron Wallace88% (32)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Renr Practice Test 11Dokumen17 halamanRenr Practice Test 11Aaron Wallace92% (12)
- April CXC Exam Plus Answers 2016 (30753)Dokumen15 halamanApril CXC Exam Plus Answers 2016 (30753)Aaron Wallace90% (10)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Admission Nurses Notes SampleDokumen3 halamanAdmission Nurses Notes SampleAaron Wallace88% (8)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Phelebotomy Answers 01 2018Dokumen61 halamanPhelebotomy Answers 01 2018Aaron Wallace100% (1)
- Scan0010 RotatedDokumen12 halamanScan0010 RotatedAaron Wallace100% (3)
- Renr Review Program 2016Dokumen8 halamanRenr Review Program 2016Aaron Wallace100% (2)
- Key April 2001 Paper 3Dokumen8 halamanKey April 2001 Paper 3Aaron WallaceBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Percussion and Auscultation: by DR - Vidhu Mittal Junior Resident Deptt. of Chest and TBDokumen87 halamanPercussion and Auscultation: by DR - Vidhu Mittal Junior Resident Deptt. of Chest and TBChiradip Mallick100% (1)
- Pulmonary Tuberculosis Case PresentationDokumen71 halamanPulmonary Tuberculosis Case PresentationSimeonDomingoTorresSy100% (4)
- Detailed Lesson PlanDokumen48 halamanDetailed Lesson PlanNaisy Magalona100% (2)
- Apirl 2001 Paper 2 (CL)Dokumen15 halamanApirl 2001 Paper 2 (CL)Aaron Wallace100% (1)
- Vascular Disorder Case StudyDokumen3 halamanVascular Disorder Case StudyAaron Wallace100% (1)
- Nurs Council TopicsDokumen1 halamanNurs Council TopicsAaron Wallace100% (1)
- Asthma MedicationsDokumen3 halamanAsthma MedicationsAaron WallaceBelum ada peringkat
- What Is AdpieDokumen5 halamanWhat Is AdpieAaron WallaceBelum ada peringkat
- Angina ManagementDokumen14 halamanAngina ManagementAaron WallaceBelum ada peringkat
- 1503 KJSDLJFLSDF X10Dokumen219 halaman1503 KJSDLJFLSDF X10Aaron WallaceBelum ada peringkat
- A Kestrel For A Knave - WikipediaDokumen26 halamanA Kestrel For A Knave - WikipediaAaron WallaceBelum ada peringkat
- Asthma MedicationsDokumen3 halamanAsthma MedicationsAaron WallaceBelum ada peringkat
- Psychology TheoriesDokumen7 halamanPsychology TheoriesAaron WallaceBelum ada peringkat
- Cardiac System MedicationsDokumen4 halamanCardiac System MedicationsfranjoyBelum ada peringkat
- Dry Swabs: Diascan StripsDokumen5 halamanDry Swabs: Diascan StripsAaron WallaceBelum ada peringkat
- Hint For AdmissionDokumen5 halamanHint For AdmissionAaron WallaceBelum ada peringkat
- International Women Day 2017Dokumen1 halamanInternational Women Day 2017Aaron WallaceBelum ada peringkat
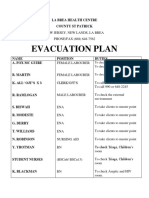
- Evacuation Plan: La Brea Health Centre County ST PatrickDokumen2 halamanEvacuation Plan: La Brea Health Centre County ST PatrickAaron WallaceBelum ada peringkat
- Labels For WardsDokumen8 halamanLabels For WardsAaron WallaceBelum ada peringkat
- October 2000 Paper 4Dokumen14 halamanOctober 2000 Paper 4Aaron Wallace100% (1)
- April 1999 Paper 1 Clinical Nursing Essay - Type Test Items: Scenario 1 Item 1Dokumen10 halamanApril 1999 Paper 1 Clinical Nursing Essay - Type Test Items: Scenario 1 Item 1Aaron WallaceBelum ada peringkat
- Bronchial AshthmaDokumen116 halamanBronchial Ashthmashaikh shabistaBelum ada peringkat
- Respiratory System: Zahra Anggita PratiwiDokumen36 halamanRespiratory System: Zahra Anggita PratiwizahraanggitaBelum ada peringkat
- Sains Tingkatan 3: Science Form 3Dokumen27 halamanSains Tingkatan 3: Science Form 3Nadzirah RedzuanBelum ada peringkat
- Measurements in Radiology Made Easy® PDFDokumen213 halamanMeasurements in Radiology Made Easy® PDFsalah subbah100% (2)
- Anatomy ShortcutDokumen73 halamanAnatomy ShortcutHARSHBelum ada peringkat
- Breathing and Exchange of Gases BIOLOGY CLASS 11Dokumen6 halamanBreathing and Exchange of Gases BIOLOGY CLASS 11AvinashBelum ada peringkat
- Anatomy Study OutlineDokumen32 halamanAnatomy Study OutlineJustine Val RevalidaBelum ada peringkat
- Тесты На Руб.3к ОМ ПЕД АнглDokumen25 halamanТесты На Руб.3к ОМ ПЕД АнглСымбат КулдасоваBelum ada peringkat
- B Inggris Halim NCP Asma BronchialDokumen28 halamanB Inggris Halim NCP Asma BronchialAbdul HlmBelum ada peringkat
- Biology N5 Past Paper Questions Multicellular Organisms1Dokumen42 halamanBiology N5 Past Paper Questions Multicellular Organisms1Craig MitchellBelum ada peringkat
- Chapter 53 - Introduction To The Respiratory SystemDokumen13 halamanChapter 53 - Introduction To The Respiratory SystemJonathonBelum ada peringkat
- Respiratory TransesDokumen4 halamanRespiratory TransesAriane Shane BidoBelum ada peringkat
- BIOS1155 Outline S1 2017Dokumen19 halamanBIOS1155 Outline S1 2017JanaBelum ada peringkat
- Drugs Affecting The Body SystemDokumen3 halamanDrugs Affecting The Body SystemKhzBelum ada peringkat
- Responses To Altered Respiratory FunctionDokumen19 halamanResponses To Altered Respiratory FunctionKoleen KirstenBelum ada peringkat
- Resp System. ExamDokumen145 halamanResp System. ExamIrina CornilovBelum ada peringkat
- Acebrofilina PozziDokumen10 halamanAcebrofilina PozziAgencia FaroBelum ada peringkat
- Endotracheal IntubationDokumen17 halamanEndotracheal IntubationShiwangi Sharma100% (1)
- Naturopathy in Respiratory Diseases FinalDokumen42 halamanNaturopathy in Respiratory Diseases FinalAmshumanBelum ada peringkat
- Chest X-Ray Fundamentals: Dr. Emad EfatDokumen241 halamanChest X-Ray Fundamentals: Dr. Emad EfatRutvik Shah100% (1)
- Recognizing Interstitial Versus Airspace Disease: in Slide Show Mode, Advance The Slides by Pressing The SpacebarDokumen32 halamanRecognizing Interstitial Versus Airspace Disease: in Slide Show Mode, Advance The Slides by Pressing The SpacebarCheska TumulakBelum ada peringkat
- Chest X-Ray Interpretation (Not Just Black and White) PDFDokumen8 halamanChest X-Ray Interpretation (Not Just Black and White) PDFVincent WesleyBelum ada peringkat
- 6th Body Systems Packet WORKSHEETSDokumen39 halaman6th Body Systems Packet WORKSHEETSElizabeth Alvarez100% (1)
- Internal Diseases Propedeutics Part I. Diagnostics of Pulmonary Diseases PDFDokumen94 halamanInternal Diseases Propedeutics Part I. Diagnostics of Pulmonary Diseases PDFYashwanth vBelum ada peringkat
- PBL Case - 2Dokumen14 halamanPBL Case - 2Jerin XavierBelum ada peringkat
- 1ST QUARTER SCI Answer KeyDokumen3 halaman1ST QUARTER SCI Answer KeyGessel Adlaon100% (1)
- Lung CancerDokumen4 halamanLung CancerÄbegail Cuanan Palang تBelum ada peringkat