Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- 10 Books For Your ADHD Library PDFDokumen1 halaman10 Books For Your ADHD Library PDFMitali Sharma100% (1)
- Luise Hay Symptoms ListDokumen12 halamanLuise Hay Symptoms Listmaviladin100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Renal - Goljan SlidesDokumen29 halamanRenal - Goljan SlidesJoan ChoiBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Entity EHS Incident ReportDokumen5 halamanEntity EHS Incident ReportwritemeyouBelum ada peringkat
- DD Pruritus AniDokumen18 halamanDD Pruritus Anie.x.oBelum ada peringkat
- Final Major Clinical Case Study Online VersionDokumen14 halamanFinal Major Clinical Case Study Online Versionapi-282107708Belum ada peringkat
- Philippine Clean Air Act of 1999Dokumen87 halamanPhilippine Clean Air Act of 1999Kei Samson100% (20)
- Heart Disease in Pregnancy: Mohana PreeshaDokumen50 halamanHeart Disease in Pregnancy: Mohana PreeshaChuks LeviBelum ada peringkat
- Schizophrenia UndifferentiatedDokumen88 halamanSchizophrenia UndifferentiatedHanya Bint Potawan75% (4)
- Dr. HY Peds Shelf Parts 1 & 2Dokumen22 halamanDr. HY Peds Shelf Parts 1 & 2Emanuella GomezBelum ada peringkat
- Medical Terminologies and AbbreviationDokumen4 halamanMedical Terminologies and AbbreviationHana LunariaBelum ada peringkat
- PTB Case-StudyDokumen64 halamanPTB Case-StudyBeverly DatuBelum ada peringkat
- Morphology Of The Pada Asc By Dr. Suresh Chandra MishraDokumen12 halamanMorphology Of The Pada Asc By Dr. Suresh Chandra Mishraadya_tripathiBelum ada peringkat
- Bailey CH 4 No 91-120Dokumen58 halamanBailey CH 4 No 91-120Withia WtBelum ada peringkat
- Bailey CH 4 No 91-120Dokumen58 halamanBailey CH 4 No 91-120Withia WtBelum ada peringkat
- Daftar Pustaka Kss WidyaDokumen3 halamanDaftar Pustaka Kss WidyaWithia WtBelum ada peringkat
- ParatidektomiDokumen16 halamanParatidektomiWithia WtBelum ada peringkat
- ParatidektomiDokumen16 halamanParatidektomiWithia WtBelum ada peringkat
- TrakeostomiDokumen4 halamanTrakeostomiWithia WtBelum ada peringkat
- TrakeostomiDokumen4 halamanTrakeostomiWithia WtBelum ada peringkat
- Nursing Care Plan for ChickenpoxDokumen2 halamanNursing Care Plan for ChickenpoxAkeroBelum ada peringkat
- Food Poisoning Causes Precautions Diagnosis and TRDokumen4 halamanFood Poisoning Causes Precautions Diagnosis and TRghadiBelum ada peringkat
- Colon Cleansing, Cleanse - Net Colon Plaque - Mucoid PlaqueDokumen15 halamanColon Cleansing, Cleanse - Net Colon Plaque - Mucoid Plaquetigerlo75100% (1)
- Chapter 5 Prep U.odtDokumen6 halamanChapter 5 Prep U.odtLivan MartellBelum ada peringkat
- Cbki4103 Knowledge Management AssignmentDokumen14 halamanCbki4103 Knowledge Management AssignmentEmily LyeBelum ada peringkat
- Nurses Guide 2010 WEBDokumen290 halamanNurses Guide 2010 WEBSunita AbrahamBelum ada peringkat
- Outbreaks Where Food Workers Have Been Implicated in The Spread of Foodborne Disease. Part 6. Transmission and Survival of Pathogens in The Food Processing and Preparation EnvironmentDokumen18 halamanOutbreaks Where Food Workers Have Been Implicated in The Spread of Foodborne Disease. Part 6. Transmission and Survival of Pathogens in The Food Processing and Preparation EnvironmentCalidad CODITEV SACBelum ada peringkat
- Abnormal Illness BehaviorDokumen7 halamanAbnormal Illness Behavioransha2011p0% (1)
- Acute Renal Failure-Student-Rapid ReasoningDokumen4 halamanAcute Renal Failure-Student-Rapid Reasoningapi-268403950Belum ada peringkat
- CGN Pediatric 1 Lesson 2Dokumen20 halamanCGN Pediatric 1 Lesson 2okumu atanasBelum ada peringkat
- Managing Cardiorenal Syndrome in a Patient with Congestive Heart FailureDokumen18 halamanManaging Cardiorenal Syndrome in a Patient with Congestive Heart Failuredauz3017Belum ada peringkat
- Quezon's Children The 2014 Quezon Provincial Nutrition Situation Facts and FiguresDokumen32 halamanQuezon's Children The 2014 Quezon Provincial Nutrition Situation Facts and FiguresToto ParcareyBelum ada peringkat
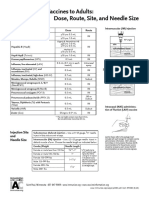
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeDokumen1 halamanAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashBelum ada peringkat
- GCP Cs DrugsDokumen13 halamanGCP Cs DrugsBel CortezBelum ada peringkat
- Sensorineural Hearing LossDokumen19 halamanSensorineural Hearing LossBenitaBelum ada peringkat
- Dental X-Ray ExamsDokumen2 halamanDental X-Ray ExamsSara Loureiro da LuzBelum ada peringkat
- Venous Blood Gas (VBG) PDFDokumen3 halamanVenous Blood Gas (VBG) PDFZamzam DomaBelum ada peringkat