Anda mungkin juga menyukai
- Clinical Pharmacy: Pathophysiology and Pharmacotherapy of Congestive Heart FailureDokumen89 halamanClinical Pharmacy: Pathophysiology and Pharmacotherapy of Congestive Heart FailureMuhammad Mustafa Ijaz100% (3)
- Preoperative AssessmentDokumen26 halamanPreoperative Assessmentkaukab azimBelum ada peringkat
- 312 ATI Critical Care MedsDokumen34 halaman312 ATI Critical Care Medslisa100% (1)
- BLOOD TRANSFUSION NotesDokumen7 halamanBLOOD TRANSFUSION NotesErl D. MelitanteBelum ada peringkat
- Management of SepsisDokumen34 halamanManagement of SepsisTamim IshtiaqueBelum ada peringkat
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingDari EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingBelum ada peringkat
- Brinster, Dermatopathology-Saunders (2011) PDFDokumen626 halamanBrinster, Dermatopathology-Saunders (2011) PDFxc_corina100% (3)
- Case Presentation DVTDokumen26 halamanCase Presentation DVTimad mokalledBelum ada peringkat
- Case 9: Deep Vein ThrombosisDokumen5 halamanCase 9: Deep Vein Thrombosisintrovoyz041Belum ada peringkat
- Renal TransplantDokumen29 halamanRenal TransplantSujith Kuttan100% (1)
- Lyme Disease Booklet1 PDFDokumen42 halamanLyme Disease Booklet1 PDFBetty100% (1)
- Therapeutic Regimens in HIVDokumen36 halamanTherapeutic Regimens in HIVGail HoadBelum ada peringkat
- Chronic Subdural HematomaDokumen21 halamanChronic Subdural Hematomamarc_caronan100% (2)
- F 360Dokumen6 halamanF 360اسعد عبد الحميد50% (2)
- Pathophysiology of Coronary Artery Disease: Basic Science For CliniciansDokumen8 halamanPathophysiology of Coronary Artery Disease: Basic Science For CliniciansZaenal AhmadBelum ada peringkat
- Carnitine DeficiencyDokumen21 halamanCarnitine Deficiencykiedd_04100% (1)
- CHEST Guidelines for VTE Antithrombotic Therapy DurationDokumen20 halamanCHEST Guidelines for VTE Antithrombotic Therapy DurationnadyasuwayviaBelum ada peringkat
- Pre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIDokumen25 halamanPre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIFatima MBelum ada peringkat
- Pediatric Hematology Oncology Ward Officer HandbookDokumen40 halamanPediatric Hematology Oncology Ward Officer HandbookAnonymous FSUnLYr4yBelum ada peringkat
- Breast History PDFDokumen9 halamanBreast History PDFApurv GuptaBelum ada peringkat
- Lecture & Review Guide in HEMATOLOGY 1 & 2 (COMPLETE)Dokumen58 halamanLecture & Review Guide in HEMATOLOGY 1 & 2 (COMPLETE)Kirt Anonuevo100% (3)
- Peptic Ulcer DiseaseDokumen4 halamanPeptic Ulcer DiseaseWidyan Muchzadi AkbarBelum ada peringkat
- Hepatitis BDokumen12 halamanHepatitis BEmicar TecBelum ada peringkat
- Blood TransfusionDokumen29 halamanBlood TransfusionNonu Kims100% (1)
- Casepresentationondvt1 200731074511Dokumen21 halamanCasepresentationondvt1 200731074511alvin.de.fieryBelum ada peringkat
- Deep Venous ThrombosisDokumen35 halamanDeep Venous ThrombosisDaisy WijayaBelum ada peringkat
- DVT by DR KabareDokumen24 halamanDVT by DR KabareAustine OdhiamboBelum ada peringkat
- Thromboembolic DisordersDokumen6 halamanThromboembolic DisordersadiBelum ada peringkat
- 7- case - parasiticDokumen18 halaman7- case - parasitickoteshwara raoBelum ada peringkat
- Vanco PRDokumen22 halamanVanco PRapi-647244341Belum ada peringkat
- CBD 1 Leukemia+LymphomaDokumen59 halamanCBD 1 Leukemia+LymphomaWan Razin Wan HassanBelum ada peringkat
- Thrombophilia: Duha Alharbi, MD InternDokumen30 halamanThrombophilia: Duha Alharbi, MD InternabrarBelum ada peringkat
- DVT 141203103638 Conversion Gate01Dokumen57 halamanDVT 141203103638 Conversion Gate01YantoBelum ada peringkat
- Coagulation Disorders in PregnancyDokumen20 halamanCoagulation Disorders in PregnancyHannaTashiaClaudiaBelum ada peringkat
- Medical Terminology, Hospital Room and Hospital TeamDokumen43 halamanMedical Terminology, Hospital Room and Hospital TeamFajriyatul KamalBelum ada peringkat
- Pediatric Hematology Oncology Ward Officer HandbookDokumen40 halamanPediatric Hematology Oncology Ward Officer HandbookLetchumana KrishnanBelum ada peringkat
- Anti Cancer DrugsDokumen29 halamanAnti Cancer DrugsFrances RamosBelum ada peringkat
- Congenitally-Acquired Advanced Hiv With Ois: Medical and Social ComplexitiesDokumen25 halamanCongenitally-Acquired Advanced Hiv With Ois: Medical and Social ComplexitiesKing MazingaBelum ada peringkat
- Deep Vein ThrombosisDokumen5 halamanDeep Vein Thrombosisampogison08Belum ada peringkat
- Comprehensive Nursing Care in Hematopoietic Stem Cell TransplantationDokumen47 halamanComprehensive Nursing Care in Hematopoietic Stem Cell TransplantationRajani Singh BaghelBelum ada peringkat
- Preoperative and Postoperative Care of Surgical Patient ModifiedDokumen68 halamanPreoperative and Postoperative Care of Surgical Patient ModifiedJohn Wesley OmbogoBelum ada peringkat
- Issues in The Diagnosis and Management of Thombocytopenic DisordersDokumen45 halamanIssues in The Diagnosis and Management of Thombocytopenic Disorderspeter_mrBelum ada peringkat
- Anticoagulants: Julene FunkDokumen25 halamanAnticoagulants: Julene FunkJulieBelum ada peringkat
- VTE Prophylaxis - COVID-19 - New SLCH. June2021Dokumen4 halamanVTE Prophylaxis - COVID-19 - New SLCH. June2021Chenuri Annamarie RanasingheBelum ada peringkat
- Reviewer 2Dokumen15 halamanReviewer 2chaSeph100% (2)
- Kuliah Thrombosis 2015 NNDokumen39 halamanKuliah Thrombosis 2015 NNBeladiena Citra SiregarBelum ada peringkat
- Case Presentation MineDokumen30 halamanCase Presentation MineAshman AshBelum ada peringkat
- Drugs Used in Cardiovascular SystemDokumen57 halamanDrugs Used in Cardiovascular SystemSandeep ChaudharyBelum ada peringkat
- In The Clinicrisk Identification &surgicalcomplicationsamaso Myear4Dokumen40 halamanIn The Clinicrisk Identification &surgicalcomplicationsamaso Myear4danielBelum ada peringkat
- VTE Deep Vein Thrombosis Pulmonary Embolism: Wong Cai Hui Supervisor: DR PradeepDokumen75 halamanVTE Deep Vein Thrombosis Pulmonary Embolism: Wong Cai Hui Supervisor: DR PradeepALIF HAIQAL MOHD HUSSEINBelum ada peringkat
- Ante-Partum HaemorrhageDokumen42 halamanAnte-Partum HaemorrhageSerenna DehalooBelum ada peringkat
- Care of Patients With Cancer of The LungsDokumen20 halamanCare of Patients With Cancer of The LungsJumar Vallo ValdezBelum ada peringkat
- Venous Thromboembolism in Urologic Surgery: Prophylaxis, Diagnosis and TreatmentDokumen25 halamanVenous Thromboembolism in Urologic Surgery: Prophylaxis, Diagnosis and TreatmentapheatBelum ada peringkat
- Rivaroxaban Resolves PICC Clot Faster Than WarfarinDokumen7 halamanRivaroxaban Resolves PICC Clot Faster Than WarfarinDiego TonelloBelum ada peringkat
- Anticoagulations in Surgery: Sharifah Naiemah BT Syed MansorDokumen20 halamanAnticoagulations in Surgery: Sharifah Naiemah BT Syed MansorSharifah NaiemahBelum ada peringkat
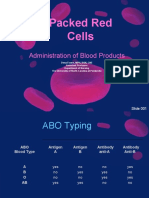
- Packed Red Cells: Administration of Blood ProductsDokumen36 halamanPacked Red Cells: Administration of Blood ProductsRj SantosBelum ada peringkat
- Venous ThromboemboslimDokumen22 halamanVenous ThromboemboslimTitusBelum ada peringkat
- Periprocedural Management With Antithrombotic Therapy Adult Inpatient Ambulatory Guideline 20201029Dokumen14 halamanPeriprocedural Management With Antithrombotic Therapy Adult Inpatient Ambulatory Guideline 20201029Joanne HoBelum ada peringkat
- LMWH QML 06Dokumen7 halamanLMWH QML 06pd7qmlBelum ada peringkat
- Antiretroviral TreatmentDokumen32 halamanAntiretroviral TreatmentStanley Tatenda MukonoBelum ada peringkat
- Prolonged ICU StayDokumen80 halamanProlonged ICU StayLady AngodBelum ada peringkat
- Early Warning ScoresDokumen14 halamanEarly Warning ScoresmuchtarBelum ada peringkat
- Upper GI BleedDokumen50 halamanUpper GI BleedNiladri BanerjeeBelum ada peringkat
- Consider Abdominal Compartment Syndrome in Patients With Refractory HypotensionDokumen26 halamanConsider Abdominal Compartment Syndrome in Patients With Refractory HypotensionHari AdityonugrohoBelum ada peringkat
- Principles of Gynecological Surgeries 1Dokumen127 halamanPrinciples of Gynecological Surgeries 1Mohammad AlrefaiBelum ada peringkat
- Anaesthesia For A Patient With Coagulation DisorderDokumen33 halamanAnaesthesia For A Patient With Coagulation DisorderNdenwaneku OkuwaBelum ada peringkat
- Khan PresentationDokumen18 halamanKhan Presentationapi-648757084Belum ada peringkat
- Blood TransfusionDokumen20 halamanBlood TransfusionRaymund Christopher Dela PeñaBelum ada peringkat
- Goljan - Integrated Pathology Notes PDFDokumen60 halamanGoljan - Integrated Pathology Notes PDFIsaac JacksBelum ada peringkat
- Goljan - High Yield Questions For USMLEDokumen36 halamanGoljan - High Yield Questions For USMLEMustafa MenemBelum ada peringkat
- DVT PresentationDokumen15 halamanDVT PresentationIsaac Jacks100% (1)
- DVT PresentationDokumen15 halamanDVT PresentationIsaac Jacks100% (1)
- Plastic's Presentation-Skin GraftingDokumen14 halamanPlastic's Presentation-Skin GraftingIsaac JacksBelum ada peringkat
- Isaac Jacks-Concert Report 1Dokumen4 halamanIsaac Jacks-Concert Report 1Isaac JacksBelum ada peringkat
- BP6 15depression PDFDokumen75 halamanBP6 15depression PDFada ramosBelum ada peringkat
- Drug NorvascDokumen1 halamanDrug NorvascSrkocherBelum ada peringkat
- Dermatology Study Guide 2021Dokumen5 halamanDermatology Study Guide 2021Osmo SisBelum ada peringkat
- Augenblickdiagnos Campbell1998 PDFDokumen8 halamanAugenblickdiagnos Campbell1998 PDFFrancoBelum ada peringkat
- Benign Breast Diseases29.7Dokumen65 halamanBenign Breast Diseases29.7api-3701915Belum ada peringkat
- Special Pathology Solved KMU SEQs by RMC StudentsDokumen145 halamanSpecial Pathology Solved KMU SEQs by RMC StudentsAamir Khan0% (1)
- Haemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)Dokumen20 halamanHaemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)shravaniBelum ada peringkat
- Bacteria PathogensDokumen7 halamanBacteria PathogensBilal Masood AhmedBelum ada peringkat
- Chronic Diarrhea - book.GITDokumen6 halamanChronic Diarrhea - book.GITAbdul QuyyumBelum ada peringkat
- Severe Peritonitis Case Report Highlights Diagnosis and Treatment of Acute PancreatitisDokumen2 halamanSevere Peritonitis Case Report Highlights Diagnosis and Treatment of Acute PancreatitisJune Faith HacheroBelum ada peringkat
- 1 كتب دكتور علام باطنه General & Cardio.whiteKnightLoveDokumen111 halaman1 كتب دكتور علام باطنه General & Cardio.whiteKnightLoveNour ShăbanBelum ada peringkat
- Sildenafil Citrate or ViagraDokumen3 halamanSildenafil Citrate or ViagraKat ZBelum ada peringkat
- Prometric Test NurseDokumen43 halamanPrometric Test NurseEdi RusmiantoBelum ada peringkat
- Clinical Pearls in NephrologyDokumen5 halamanClinical Pearls in NephrologyEdmilson R. LimaBelum ada peringkat
- Karoshi PDFDokumen6 halamanKaroshi PDFJuanito MaravillasBelum ada peringkat
- A1c in PregnancyDokumen20 halamanA1c in PregnancynandhinilpBelum ada peringkat
- Chemtrails Learn How To Protect Yourself From These Treacherous PoisonsDokumen2 halamanChemtrails Learn How To Protect Yourself From These Treacherous PoisonsDarkcastle2012Belum ada peringkat
- MS Ii MT2Dokumen11 halamanMS Ii MT2Rika MaeBelum ada peringkat
- File 18588Dokumen4 halamanFile 18588Mohammed MuthanaBelum ada peringkat
- Rina Ramayani Komplikasi SN KONIKA XVIIDokumen26 halamanRina Ramayani Komplikasi SN KONIKA XVIIirene aureliaBelum ada peringkat