Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- REBASING & RELINING DENTURES COMPLETELYDokumen18 halamanREBASING & RELINING DENTURES COMPLETELYAditya ZulfikarBelum ada peringkat
- Denture Stomatitis KP UNissula Mei 2016Dokumen53 halamanDenture Stomatitis KP UNissula Mei 2016Aditya ZulfikarBelum ada peringkat
- Dok Yusuf (Ekstraoral Radiography)Dokumen72 halamanDok Yusuf (Ekstraoral Radiography)Aditya ZulfikarBelum ada peringkat
- KP Lesi Pre Kanker Kanker Dan Efek Terapi Kanker Rongga MulutDokumen58 halamanKP Lesi Pre Kanker Kanker Dan Efek Terapi Kanker Rongga MulutAditya ZulfikarBelum ada peringkat
- Dok Rama (Functional Appliance)Dokumen36 halamanDok Rama (Functional Appliance)Aditya ZulfikarBelum ada peringkat
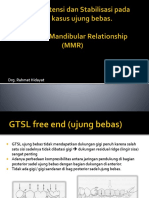
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRDokumen53 halamanDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarBelum ada peringkat
- Pengaruh Terapi CA Pada Rongga MulutDokumen24 halamanPengaruh Terapi CA Pada Rongga MulutAditya ZulfikarBelum ada peringkat
- The Oral-Systemic Connection: Understanding the Relationship Between Periodontal Disease and Systemic HealthDokumen25 halamanThe Oral-Systemic Connection: Understanding the Relationship Between Periodontal Disease and Systemic HealthAditya ZulfikarBelum ada peringkat
- Periodontal Disease and Systemic Health ConnectionDokumen25 halamanPeriodontal Disease and Systemic Health ConnectionAditya ZulfikarBelum ada peringkat
- Dok Yusuf (Ekstraoral Radiography)Dokumen72 halamanDok Yusuf (Ekstraoral Radiography)Aditya ZulfikarBelum ada peringkat
- GINGIVAL Disease KulpakDokumen61 halamanGINGIVAL Disease KulpakAditya ZulfikarBelum ada peringkat
- Komplikasi AlDokumen29 halamanKomplikasi AlAditya ZulfikarBelum ada peringkat
- DRG Ade MSLH Elderely MHSWDokumen36 halamanDRG Ade MSLH Elderely MHSWAditya ZulfikarBelum ada peringkat
- DRG Ade MSLH Elderely MHSWDokumen36 halamanDRG Ade MSLH Elderely MHSWAditya ZulfikarBelum ada peringkat
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRDokumen53 halamanDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarBelum ada peringkat
- Visual Diagnosis Oral Soft Tissue Lession in PediatricDokumen39 halamanVisual Diagnosis Oral Soft Tissue Lession in PediatricAditya ZulfikarBelum ada peringkat
- Dental AnatomyDokumen61 halamanDental AnatomyAditya ZulfikarBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Elastic Properties and Apparent Density of Human Edn. Maxilla and Mand.Dokumen6 halamanElastic Properties and Apparent Density of Human Edn. Maxilla and Mand.Mahmood E.Belum ada peringkat
- 39.anteroposterior CephalometricsDokumen40 halaman39.anteroposterior CephalometricsMariyamBelum ada peringkat
- Head and Neck - Anterior Head and Neck - LateralDokumen17 halamanHead and Neck - Anterior Head and Neck - LateralYma FeelBelum ada peringkat
- McqsDokumen12 halamanMcqssarahh100% (2)
- Comparison of 2 Comprehensive Class II Treatment Protocols Bonded Herbst and Headgear PDFDokumen10 halamanComparison of 2 Comprehensive Class II Treatment Protocols Bonded Herbst and Headgear PDFMargarida Maria LealBelum ada peringkat
- Theories of GrowthDokumen67 halamanTheories of GrowthsoujanyaBelum ada peringkat
- Schistura ThavoneiDokumen9 halamanSchistura ThavoneiSubhadra LaimayumBelum ada peringkat
- Exam Hilla 1122Dokumen4 halamanExam Hilla 1122zainBelum ada peringkat
- Accuracy of Check BiteDokumen9 halamanAccuracy of Check BiteMuhammad Shakeel KhawajaBelum ada peringkat
- Poison Apparatus and The Biting Mechanism of SnakesDokumen6 halamanPoison Apparatus and The Biting Mechanism of SnakesdikhsyaguragainBelum ada peringkat
- OSTEOMYELITIS OF JAW: PATHOGENESIS & MANAGEMENTDokumen35 halamanOSTEOMYELITIS OF JAW: PATHOGENESIS & MANAGEMENTOded KantzukerBelum ada peringkat
- Principles and Management of Panfacial TraumaDokumen43 halamanPrinciples and Management of Panfacial TraumaDR NASIMBelum ada peringkat
- Medical Term List PDFDokumen21 halamanMedical Term List PDFAntonSusantoBelum ada peringkat
- Single Visit EndodonticsDokumen6 halamanSingle Visit EndodonticsFathi BanurBelum ada peringkat
- Anchorage in Orthodontics: Understanding Resistance to Tooth MovementDokumen34 halamanAnchorage in Orthodontics: Understanding Resistance to Tooth MovementVasundhra MittalBelum ada peringkat
- Exercises in Oral Radiographic InterpretationsDokumen239 halamanExercises in Oral Radiographic InterpretationsSufaru Ciprian75% (4)
- Alveolingual SulcusDokumen8 halamanAlveolingual SulcusMrinmayee ThakurBelum ada peringkat
- Maxillary Canine Transpositions: Classification, Prevalence and TreatmentDokumen8 halamanMaxillary Canine Transpositions: Classification, Prevalence and Treatmentjohnmax100% (2)
- Dental Occlusion A Newly Proposed TetrahDokumen10 halamanDental Occlusion A Newly Proposed TetrahIlinca LupuBelum ada peringkat
- ANTHROMETRIC MEASUREMENTSDokumen11 halamanANTHROMETRIC MEASUREMENTSdrrebaBelum ada peringkat
- OinaDokumen19 halamanOinaPauline JaleaBelum ada peringkat
- Extrinsic and Intrinsic Factors in The Etiology of MalocclusionDokumen7 halamanExtrinsic and Intrinsic Factors in The Etiology of MalocclusionNavroop KaurBelum ada peringkat
- Orthopaedic ForcesDokumen43 halamanOrthopaedic ForcesminalBelum ada peringkat
- Muscles of Mastication: - DR - Asif Iqbal - 2 Year P.GDokumen85 halamanMuscles of Mastication: - DR - Asif Iqbal - 2 Year P.GSaghar AbroBelum ada peringkat
- ENT - Anatomy and Physiology of The Oral CavityDokumen3 halamanENT - Anatomy and Physiology of The Oral CavityJaybee Sarmiento100% (2)
- ArticulatorsDokumen6 halamanArticulatorsSameh Magdy Abou El-KheirBelum ada peringkat
- 5 Reqs For Occlusal StabilityDokumen2 halaman5 Reqs For Occlusal StabilityNirav MehtaBelum ada peringkat
- Dental Articulator & Face-Bow: ProsthodonticsDokumen12 halamanDental Articulator & Face-Bow: ProsthodonticsPriyanka GandhiBelum ada peringkat
- Essentials of Oral Biology PDFDokumen614 halamanEssentials of Oral Biology PDFRudra VermaBelum ada peringkat
- NEET MDS Picture Based QuestionsDokumen74 halamanNEET MDS Picture Based QuestionsAysha NazrinBelum ada peringkat