Anda mungkin juga menyukai
- Recent Advances in PhysiotherapyDari EverandRecent Advances in PhysiotherapyCecily PartridgeBelum ada peringkat
- Ijspt-Biomechanics and Pathomechanics of The Patellofemoral JointDokumen11 halamanIjspt-Biomechanics and Pathomechanics of The Patellofemoral JointDevi MigiekaBelum ada peringkat
- Management of Musculoskeletal DisordersDokumen69 halamanManagement of Musculoskeletal DisordersJSeasharkBelum ada peringkat
- Cervicovestibular Rehabilitation in Sport-Related Concussion - A Randomised Controlled TrialDokumen7 halamanCervicovestibular Rehabilitation in Sport-Related Concussion - A Randomised Controlled TrialhilmikamelBelum ada peringkat
- A Proposed Evidence-Based Shoulder Special Testing Examination Algorithm - Clinical Utility Based On A Systematic Review of The LiteratureDokumen14 halamanA Proposed Evidence-Based Shoulder Special Testing Examination Algorithm - Clinical Utility Based On A Systematic Review of The LiteratureAfonso MacedoBelum ada peringkat
- The Timed Up & Go - A Test of Basic Functional Mobility For Frail Elderly Persons. lAGSDokumen7 halamanThe Timed Up & Go - A Test of Basic Functional Mobility For Frail Elderly Persons. lAGSJose Fernando Díez ConchaBelum ada peringkat
- Balance and Vestibular Rehabilitation KitDokumen9 halamanBalance and Vestibular Rehabilitation Kitmsnobody8Belum ada peringkat
- Warning: You May Want To Look Away at Times!: Youtube VideoDokumen47 halamanWarning: You May Want To Look Away at Times!: Youtube VideoRaffy B. MabilingBelum ada peringkat
- PT Practice Guide 2004 Final Version April 05 PDFDokumen509 halamanPT Practice Guide 2004 Final Version April 05 PDFMahfud HidayatBelum ada peringkat
- Rehabilitation of Sports Injuries - Scientific BasisDokumen338 halamanRehabilitation of Sports Injuries - Scientific Basisjimitkapadia100% (3)
- LowBackPain PDFDokumen217 halamanLowBackPain PDFBugis MuslimBelum ada peringkat
- Time Code Title Author: Date: 30-07-2021Dokumen4 halamanTime Code Title Author: Date: 30-07-2021siddhartha senBelum ada peringkat
- PAE 1 Introduction To ElectrotherapyDokumen37 halamanPAE 1 Introduction To ElectrotherapyHasnat AhmedBelum ada peringkat
- Exercise Rehabilitation Assessment - Achilles Tendinopathy-1Dokumen33 halamanExercise Rehabilitation Assessment - Achilles Tendinopathy-1GordonHessellBelum ada peringkat
- 03 RehabilitationDokumen42 halaman03 RehabilitationAlexandra ComanBelum ada peringkat
- Rehabilitation of Sports InjuiresDokumen18 halamanRehabilitation of Sports InjuiresSurgicalgownBelum ada peringkat
- The Efficacy of Brotzman Physiotherapy Protocol On Pain and Knee Range of Motion in Post Surgical Total Knee Arthroplasty Subjects With ObesityDokumen6 halamanThe Efficacy of Brotzman Physiotherapy Protocol On Pain and Knee Range of Motion in Post Surgical Total Knee Arthroplasty Subjects With ObesityInternational Journal of Physiotherapy and ResearchBelum ada peringkat
- What Is PhysiotherapyDokumen61 halamanWhat Is PhysiotherapySharikh NorazrinBelum ada peringkat
- Guide To PT PracticeDokumen98 halamanGuide To PT PracticeKana AmesBelum ada peringkat
- Athletic Taping and Bracing 2Dokumen24 halamanAthletic Taping and Bracing 2Advanced Physiotherapy100% (1)
- Tetraplegia+and+Paraplegia by Ida BromleyDokumen411 halamanTetraplegia+and+Paraplegia by Ida Bromleyrdesai04100% (2)
- Resisted Isometric TestingDokumen15 halamanResisted Isometric TestingDr. Disha Rupareliya BhateBelum ada peringkat
- Rene Cailliet - Shoulder Pain PDFDokumen170 halamanRene Cailliet - Shoulder Pain PDFm alfin alfauziBelum ada peringkat
- MC Kenzie: Diagnostic, Prognostic, Therapeutic, and ProphylacticDokumen19 halamanMC Kenzie: Diagnostic, Prognostic, Therapeutic, and ProphylacticEvaBelum ada peringkat
- Course Material - Manual TherapyDokumen196 halamanCourse Material - Manual Therapypuntocom111100% (1)
- Nutrition: BY: Nur Diana Shahira & Wan Muhammad Aiman AminDokumen22 halamanNutrition: BY: Nur Diana Shahira & Wan Muhammad Aiman AminWan Amin100% (1)
- Management of Patellofemoral Pain SyndromeDokumen9 halamanManagement of Patellofemoral Pain Syndromethe M fingerBelum ada peringkat
- Basics of Soft - Tissue ExaminationDokumen32 halamanBasics of Soft - Tissue ExaminationGurudutt PaiBelum ada peringkat
- 1 Reviews Evidences HandoutDokumen25 halaman1 Reviews Evidences Handoutsefhilla putriBelum ada peringkat
- McKenzie Classification of Mechanical Spinal PainDokumen7 halamanMcKenzie Classification of Mechanical Spinal PainVictor Andrés Olivares Ibarra100% (2)
- Interferential Therapy Sept 08Dokumen8 halamanInterferential Therapy Sept 08api-19753815100% (1)
- Performing Palpation TechniquesDokumen49 halamanPerforming Palpation TechniquesTina TalmadgeBelum ada peringkat
- PathomechanicsDokumen8 halamanPathomechanicsMike B AndersonBelum ada peringkat
- Lec.01.BASIC TERMINOLOGYDokumen66 halamanLec.01.BASIC TERMINOLOGYpashaBelum ada peringkat
- The Effect of Closed Kinetic Chain Exercises And.14Dokumen7 halamanThe Effect of Closed Kinetic Chain Exercises And.14fgomez235Belum ada peringkat
- Hari Subedi Physiotherapist: Physiotherapy Equipment ChecklistDokumen7 halamanHari Subedi Physiotherapist: Physiotherapy Equipment ChecklistdinuBelum ada peringkat
- Thermoregulation During Exercise inDokumen15 halamanThermoregulation During Exercise inRicardo LeaoBelum ada peringkat
- A Home Exercise BookDokumen28 halamanA Home Exercise BookNameeta Shroff JainBelum ada peringkat
- Spasticity ManagementDokumen17 halamanSpasticity ManagementLowell QuadrosBelum ada peringkat
- Chapter 1 - Intro Current Concepts and Clinical Decision Making in Electrotherapy PDFDokumen7 halamanChapter 1 - Intro Current Concepts and Clinical Decision Making in Electrotherapy PDFTracy Magpoc0% (1)
- Diabetes and PhysiotherapyDokumen15 halamanDiabetes and Physiotherapyane2saBelum ada peringkat
- Abdominal Strain Injury AKADokumen31 halamanAbdominal Strain Injury AKAtony whartonBelum ada peringkat
- Evidenced Based Practice in Physical TherapyDokumen3 halamanEvidenced Based Practice in Physical TherapyAndrews Milton100% (1)
- Physiotherapy Scope of Practice-Article PDFDokumen3 halamanPhysiotherapy Scope of Practice-Article PDFeins_mptBelum ada peringkat
- Orthopedic Physiotherapy Assignment: 1. Patient HistoryDokumen4 halamanOrthopedic Physiotherapy Assignment: 1. Patient HistoryarushiBelum ada peringkat
- Sports Injuries - Mechanisms, Prevention and Treatment 2nd Ed - F. Fu, D. Stone Lippincott 1994) WWDokumen1.025 halamanSports Injuries - Mechanisms, Prevention and Treatment 2nd Ed - F. Fu, D. Stone Lippincott 1994) WWplatonRO100% (1)
- Biomechanics of The Knee During Closed Kinetic Chain ExercisesDokumen31 halamanBiomechanics of The Knee During Closed Kinetic Chain ExercisesJean SantosBelum ada peringkat
- Physiotherapy Technician - CTS - NSQF-4Dokumen41 halamanPhysiotherapy Technician - CTS - NSQF-4gaurav kumarBelum ada peringkat
- Straight Sprinting Is The Most Frequent Action in Goal Situatinos in Professional FootballDokumen8 halamanStraight Sprinting Is The Most Frequent Action in Goal Situatinos in Professional Footballantonio carrillo expositoBelum ada peringkat
- Stretching With Children With Cerebral Palsy What.8 PDFDokumen6 halamanStretching With Children With Cerebral Palsy What.8 PDFNurul FadhillahBelum ada peringkat
- Manual Trigger Point Therapy and Dry Needling Top 30 MusclesDokumen84 halamanManual Trigger Point Therapy and Dry Needling Top 30 MusclesManuela CormioBelum ada peringkat
- Overhead Throwing: Biomechanics and PathologyDokumen7 halamanOverhead Throwing: Biomechanics and Pathologyrapannika100% (1)
- TerapiDokumen12 halamanTerapiOleseaVerebcean100% (1)
- Achilles RuptureDokumen23 halamanAchilles RupturePhysiotherapist AliBelum ada peringkat
- Exercise to Prevent and Manage Chronic Disease Across the LifespanDari EverandExercise to Prevent and Manage Chronic Disease Across the LifespanBelum ada peringkat
- 1246 PDFDokumen4 halaman1246 PDFPrima RiyandiBelum ada peringkat
- Antibiotic Dosing Guidelines For Renal ImpairmentDokumen6 halamanAntibiotic Dosing Guidelines For Renal ImpairmentvitauxianaBelum ada peringkat
- ENTDokumen20 halamanENTGaurav BatniBelum ada peringkat
- Scorebuilders 1Dokumen43 halamanScorebuilders 1Kilopop Man60% (5)
- Active Retirement Ireland: Welcome To The New ARI NewsDokumen8 halamanActive Retirement Ireland: Welcome To The New ARI NewsWorldReachPR100% (2)
- Canine Thromboembolic Disease: A Case Study and ReviewDokumen15 halamanCanine Thromboembolic Disease: A Case Study and ReviewJudy ZedalisBelum ada peringkat
- Isolation 1Dokumen16 halamanIsolation 1Surabhi RairamBelum ada peringkat
- Wound Healer 31Dokumen19 halamanWound Healer 31Alexandrina Cornelia AngelescuBelum ada peringkat
- Preliminary Test of Phytochemical Screening of Crude Ethanolic and Aqueous Extract of Moringa Pterygosperma GaertnDokumen3 halamanPreliminary Test of Phytochemical Screening of Crude Ethanolic and Aqueous Extract of Moringa Pterygosperma GaertnFadhil Muhammad AwaluddinBelum ada peringkat
- PL1101E - Chapter 6 NotesDokumen3 halamanPL1101E - Chapter 6 NotesMichael BBelum ada peringkat
- Chen 2018Dokumen7 halamanChen 2018Victor MocioiuBelum ada peringkat
- DHQ Flowcharts v2.0Dokumen49 halamanDHQ Flowcharts v2.0SabirAli SayyedBelum ada peringkat
- Placenta Abruptio - Topic OverviewDokumen8 halamanPlacenta Abruptio - Topic OverviewLei AbellarBelum ada peringkat
- Towards Improving post-SSRI Sexual Dysfunction by Using Nutriceuticals: Lessons From A Case Study - Calabrò 2019Dokumen8 halamanTowards Improving post-SSRI Sexual Dysfunction by Using Nutriceuticals: Lessons From A Case Study - Calabrò 2019Julio JuarezBelum ada peringkat
- Spiraldynamik SkolioseDokumen5 halamanSpiraldynamik SkolioseLauren WrightBelum ada peringkat
- Jill Getchell, BS, CCP, LCP, LPNDokumen115 halamanJill Getchell, BS, CCP, LCP, LPNapi-301270014Belum ada peringkat
- Pediatric G.I Disorders FinalDokumen53 halamanPediatric G.I Disorders FinalRashid Hussain0% (1)
- New Problem StatementDokumen2 halamanNew Problem Statementrenuka rathore100% (2)
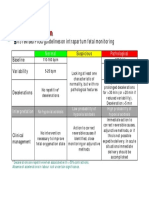
- CTG Classification PDFDokumen1 halamanCTG Classification PDFganotBelum ada peringkat
- Update 2020 - Draft Baru 30 5 2019Dokumen9 halamanUpdate 2020 - Draft Baru 30 5 2019Ridho Naibaho NaibahoBelum ada peringkat
- Yagyopathy: Applications of Yajna For Healing Amidst The Fascinating AchievementsDokumen21 halamanYagyopathy: Applications of Yajna For Healing Amidst The Fascinating AchievementsNamrata75100% (1)
- This History of Repertories - RepertoryDokumen2 halamanThis History of Repertories - RepertoryShivBalakChauhanBelum ada peringkat
- Blood TransfusionDokumen48 halamanBlood TransfusionJhade RelletaBelum ada peringkat
- Abilify, An Antipsychotic DrugDokumen4 halamanAbilify, An Antipsychotic DrugAdam RodriguezBelum ada peringkat
- Surgery Guide BookDokumen26 halamanSurgery Guide BookRaden GungunBelum ada peringkat
- Beta BlockersDokumen2 halamanBeta BlockersmetkosdBelum ada peringkat
- Malignant Soft Tissue TumorsDokumen21 halamanMalignant Soft Tissue TumorsEva GustianiBelum ada peringkat
- Health Teaching PlanDokumen4 halamanHealth Teaching PlanRene John Francisco80% (5)
- Fundamentals Exam ADokumen38 halamanFundamentals Exam APatrice Miller100% (3)
- Kim Ngoc Nguyen (21859825) - Reflective EssayDokumen1 halamanKim Ngoc Nguyen (21859825) - Reflective EssaynkngocBelum ada peringkat