Anda mungkin juga menyukai
- Mannino Heiberger FedorovDokumen18 halamanMannino Heiberger Fedorovxavo_27Belum ada peringkat
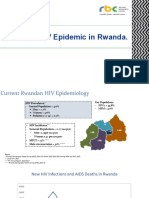
- State of HIV Epidemic in RwandaDokumen17 halamanState of HIV Epidemic in RwandaNshimiyimana Jean ClaudeBelum ada peringkat
- Survey Sampling Theory and ApplicationsDari EverandSurvey Sampling Theory and ApplicationsPenilaian: 4.5 dari 5 bintang4.5/5 (3)
- Statistical MethodsDokumen29 halamanStatistical MethodsWalter Arriola100% (1)
- Rwanda Pricelist-11-11-2016Dokumen85 halamanRwanda Pricelist-11-11-2016BISHWEKA CherifBelum ada peringkat
- ED Analyze Phase: International School of Business SfaxDokumen20 halamanED Analyze Phase: International School of Business SfaxMahdi KhemakhemBelum ada peringkat
- Establishment of Reference IntervalsDokumen42 halamanEstablishment of Reference IntervalsSparrowBelum ada peringkat
- Minimum Sample For Diagnostic TestDokumen6 halamanMinimum Sample For Diagnostic TestLulu DjalilBelum ada peringkat
- IVT Network - Statistical Analysis in Analytical Method Validation - 2014-07-10Dokumen11 halamanIVT Network - Statistical Analysis in Analytical Method Validation - 2014-07-10Jose Luis Huaman100% (1)
- Linearity of Calibration Curves For Analytical MethodsDokumen21 halamanLinearity of Calibration Curves For Analytical MethodsAna Carolina SantosBelum ada peringkat
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDokumen21 halamanWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistskarncmuBelum ada peringkat
- Analytical Validation SOP-0014Dokumen10 halamanAnalytical Validation SOP-0014os4185100% (3)
- What's New in CLSI EP15-A3: User Verification of Precision and Estimation of Bias Approved Guideline - Third EditionDokumen4 halamanWhat's New in CLSI EP15-A3: User Verification of Precision and Estimation of Bias Approved Guideline - Third Editionjrlr65Belum ada peringkat
- A2 116 2014 PDFDokumen10 halamanA2 116 2014 PDFbenlahnecheBelum ada peringkat
- Overview Of Bayesian Approach To Statistical Methods: SoftwareDari EverandOverview Of Bayesian Approach To Statistical Methods: SoftwareBelum ada peringkat
- Critical Appraisal 2017Dokumen65 halamanCritical Appraisal 2017Fransiscus RivaldyBelum ada peringkat
- EconometricsFinal Group 4Dokumen32 halamanEconometricsFinal Group 4Kripa MehtaBelum ada peringkat
- Method Validation and VerificationDokumen54 halamanMethod Validation and VerificationfadliBelum ada peringkat
- Bioavailability and Bioequivalence: By: Kris May Lyn A. RamosDokumen77 halamanBioavailability and Bioequivalence: By: Kris May Lyn A. RamosValar Morghulis100% (1)
- Journal Analytical Balance 1 PDFDokumen2 halamanJournal Analytical Balance 1 PDFJeremy Gordon100% (1)
- Interpretation of Data by SurakshyaDokumen13 halamanInterpretation of Data by Surakshyasubash karkiBelum ada peringkat
- Reporting Standardization in Pathology: Elizabeth H Hammond MD FCAPDokumen29 halamanReporting Standardization in Pathology: Elizabeth H Hammond MD FCAPCristi PopescuBelum ada peringkat
- 02.12.2014 - Sample Size Survival Analysis Common Issues in Data AnalysisDokumen60 halaman02.12.2014 - Sample Size Survival Analysis Common Issues in Data AnalysisAnna SeeBelum ada peringkat
- Probabilistic Methods in Geotechnical Engineering PDFDokumen17 halamanProbabilistic Methods in Geotechnical Engineering PDFBagusBelum ada peringkat
- Mms Testing of HypothesisDokumen69 halamanMms Testing of HypothesisKenneth MathewsBelum ada peringkat
- Linearity of Calibration Curves For Analytical Methods: A Review of Criteria For Assessment of Method ReliabilityDokumen20 halamanLinearity of Calibration Curves For Analytical Methods: A Review of Criteria For Assessment of Method ReliabilityAhmed AtefBelum ada peringkat
- Statistical Thinking for Non-Statisticians in Drug RegulationDari EverandStatistical Thinking for Non-Statisticians in Drug RegulationBelum ada peringkat
- Clinical Trial 3Dokumen20 halamanClinical Trial 3Emil LasulikaBelum ada peringkat
- Research MethodsDokumen103 halamanResearch Methodsbirtukankassa99Belum ada peringkat
- Smart Business Problems and Analytical Hints in Cancer ResearchDari EverandSmart Business Problems and Analytical Hints in Cancer ResearchBelum ada peringkat
- Method ValidationDokumen27 halamanMethod Validationsima simaBelum ada peringkat
- Bio Medical Principles of AnalysisDokumen44 halamanBio Medical Principles of AnalysisLavish ChauhanBelum ada peringkat
- Introduction To Non Parametric Methods Through R SoftwareDari EverandIntroduction To Non Parametric Methods Through R SoftwareBelum ada peringkat
- Industrial Training Module For HPLC Instruments PDFDokumen4 halamanIndustrial Training Module For HPLC Instruments PDFSpeedking RathourBelum ada peringkat
- Day 3 Session 1 Module 6 Chi Square TestDokumen15 halamanDay 3 Session 1 Module 6 Chi Square TestSanjay PudasainiBelum ada peringkat
- Establishing Acceptance Criteria For Analytical MethodsDokumen8 halamanEstablishing Acceptance Criteria For Analytical MethodsgcbBelum ada peringkat
- Special Internal Quality ControlDokumen98 halamanSpecial Internal Quality ControlDEEPAK SINGH SANGWANBelum ada peringkat
- Binary Data Analysis of Randomized Clinical Trials with NoncomplianceDari EverandBinary Data Analysis of Randomized Clinical Trials with NoncomplianceBelum ada peringkat
- Model For The Computation of Cutoff For "In House " or Modified TestsDokumen17 halamanModel For The Computation of Cutoff For "In House " or Modified TestsPaulo PereiraBelum ada peringkat
- Method Validation - QCDokumen39 halamanMethod Validation - QCteppie0917Belum ada peringkat
- CLL PatientReportDokumen7 halamanCLL PatientReportHassan Sarfraz AliBelum ada peringkat
- Phase II Research Organization DocumentDokumen4 halamanPhase II Research Organization Documentapi-633102425Belum ada peringkat
- 16th Laboratory and Outreach Survey Findings Final Cle10 v5-3Dokumen27 halaman16th Laboratory and Outreach Survey Findings Final Cle10 v5-3Expert TutoraBelum ada peringkat
- Romanach PresentationDokumen37 halamanRomanach PresentationAlejandro Romero ValenciaBelum ada peringkat
- MaurersummaryDokumen11 halamanMaurersummaryapi-243468464Belum ada peringkat
- Lecture 8 Compatibility ModeDokumen19 halamanLecture 8 Compatibility ModeChâu TrầnBelum ada peringkat
- Estimating Sample Size and Power: Applications and ExamplesDokumen10 halamanEstimating Sample Size and Power: Applications and ExamplesMaudy Lila KartikaBelum ada peringkat
- APHL Molecular Workshop 2020 Lee How To Validate A Molecular AssayDokumen32 halamanAPHL Molecular Workshop 2020 Lee How To Validate A Molecular AssayEthan LynnBelum ada peringkat
- Patient Health Assist: Under The Guidance ofDokumen30 halamanPatient Health Assist: Under The Guidance ofRajesh KumarBelum ada peringkat
- FA Lecture 3Dokumen31 halamanFA Lecture 3jm luBelum ada peringkat
- Lesson 5 PPTDokumen16 halamanLesson 5 PPTAiza CeciliaBelum ada peringkat
- How to Scale-Up a Wet Granulation End Point ScientificallyDari EverandHow to Scale-Up a Wet Granulation End Point ScientificallyPenilaian: 4 dari 5 bintang4/5 (1)
- Analytical Validation and Points For Discussion: Julia Tait Lathrop, PHDDokumen46 halamanAnalytical Validation and Points For Discussion: Julia Tait Lathrop, PHDAlicia GarcíaBelum ada peringkat
- ComputerDokumen17 halamanComputerAyeshaBelum ada peringkat
- Personalized Medicine - Future Impact Pharma Industry PerspectiveDokumen16 halamanPersonalized Medicine - Future Impact Pharma Industry PerspectivethebigpicturecoilBelum ada peringkat
- Intra Operative Aspiration PneumoniaDokumen2 halamanIntra Operative Aspiration PneumoniaLovelydePerioBelum ada peringkat
- Sample Size Guideline For Correlation Analysis: World Journal of Social Science Research March 2016Dokumen11 halamanSample Size Guideline For Correlation Analysis: World Journal of Social Science Research March 2016Nadila mudeaBelum ada peringkat
- Method Validation Tcm45-9295Dokumen18 halamanMethod Validation Tcm45-9295Ahmed AboamerBelum ada peringkat
- Change Management: TCS InternalDokumen17 halamanChange Management: TCS Internalxavo_27Belum ada peringkat
- Predictive Modeling: Logistic RegressionDokumen13 halamanPredictive Modeling: Logistic Regressionxavo_27Belum ada peringkat
- Broad Definition:: Competency NameDokumen7 halamanBroad Definition:: Competency Namexavo_27Belum ada peringkat
- Conditions Générales D'assurance 1.7.2016 ANGDokumen40 halamanConditions Générales D'assurance 1.7.2016 ANGxavo_27Belum ada peringkat
- Day9 hrp223 20081111Dokumen51 halamanDay9 hrp223 20081111xavo_27Belum ada peringkat
- Accessing Data: SAS Base Programming For SAS 9 ExamDokumen6 halamanAccessing Data: SAS Base Programming For SAS 9 Examxavo_27Belum ada peringkat
- Reduce The File Size of A Picture PDFDokumen5 halamanReduce The File Size of A Picture PDFMayur SiddharthBelum ada peringkat
- 2015 12 ReportDokumen69 halaman2015 12 Reportxavo_27Belum ada peringkat
- DPTX 2012 2 11320 0 378365 0 140374Dokumen71 halamanDPTX 2012 2 11320 0 378365 0 140374xavo_27Belum ada peringkat
- Info Maps PDFDokumen68 halamanInfo Maps PDFtempBelum ada peringkat
- Subject CT1 Financial Mathematics Core Technical Syllabus: For The 2014 ExamsDokumen6 halamanSubject CT1 Financial Mathematics Core Technical Syllabus: For The 2014 Examsapple8whiteBelum ada peringkat
- SCRinGI EnglandVerrallDokumen76 halamanSCRinGI EnglandVerrallankaradBelum ada peringkat
- Triangle Free ReservingDokumen76 halamanTriangle Free ReservingKostasSoufrasBelum ada peringkat
- The Actuary'S Free Study Guide For Exam 4 / Exam C: G. Stolyarov IiDokumen430 halamanThe Actuary'S Free Study Guide For Exam 4 / Exam C: G. Stolyarov IiKostasSoufrasBelum ada peringkat
- Our - Ethics - For - You PDFDokumen6 halamanOur - Ethics - For - You PDFxavo_27Belum ada peringkat
- Predictive Modeling: Logistic RegressionDokumen13 halamanPredictive Modeling: Logistic Regressionxavo_27Belum ada peringkat
- Edu General Insurance InfographicDokumen1 halamanEdu General Insurance Infographicxavo_27Belum ada peringkat
- Edu General Insurance InfographicDokumen1 halamanEdu General Insurance Infographicxavo_27Belum ada peringkat
- Productflyer - 978 3 642 05155 5 PDFDokumen1 halamanProductflyer - 978 3 642 05155 5 PDFxavo_27Belum ada peringkat
- Proc SgplotDokumen20 halamanProc SgplotAlok Kumar SinghBelum ada peringkat
- HW1 CommentsDokumen1 halamanHW1 Commentsxavo_27Belum ada peringkat
- 133 Survey Question AnswersDokumen33 halaman133 Survey Question Answersxavo_27Belum ada peringkat
- Journal of Statistical Software: SIMEX R Package For Accelerated Failure Time Models With Covariate Measurement ErrorDokumen14 halamanJournal of Statistical Software: SIMEX R Package For Accelerated Failure Time Models With Covariate Measurement Errorxavo_27Belum ada peringkat
- Pricing and Reserving in The General Insurance IndustryDokumen10 halamanPricing and Reserving in The General Insurance Industryxavo_27Belum ada peringkat
- Survival Analysis in R PDFDokumen16 halamanSurvival Analysis in R PDFmarciodoamaralBelum ada peringkat
- SAS CC Primer Semestre 2018Dokumen2 halamanSAS CC Primer Semestre 2018xavo_27Belum ada peringkat
- Research Ibnr Report 2009Dokumen202 halamanResearch Ibnr Report 2009Teguh PermanaBelum ada peringkat
- PharmaSUG 2014 PO17 PDFDokumen11 halamanPharmaSUG 2014 PO17 PDFxavo_27Belum ada peringkat
- What Is Empirical Research Study - (Examples - Method)Dokumen9 halamanWhat Is Empirical Research Study - (Examples - Method)Samuel AbebawBelum ada peringkat
- Dissertation CSR in The Cosmetic IndustryDokumen16 halamanDissertation CSR in The Cosmetic IndustryChris MwangiBelum ada peringkat
- Undergraduate Program - Cross Enroll Courses - AMA OEdDokumen7 halamanUndergraduate Program - Cross Enroll Courses - AMA OEdUnsolicited CommentBelum ada peringkat
- Research in MapehDokumen4 halamanResearch in MapehEmelrose LL MacedaBelum ada peringkat
- Tracer Study of Business GraduatesDokumen15 halamanTracer Study of Business GraduatesMary Ella Vega GonzagaBelum ada peringkat
- STRAMADokumen22 halamanSTRAMAMilaine ZilabboBelum ada peringkat
- Wako Thesis Proposal 1Dokumen21 halamanWako Thesis Proposal 1Nagesso GodanaBelum ada peringkat
- Game Theory - Wikipedia, The Free Encyclopedia PDFDokumen25 halamanGame Theory - Wikipedia, The Free Encyclopedia PDFHenryBelum ada peringkat
- RPS Quantitative ResearchDokumen3 halamanRPS Quantitative ResearchrahmaBelum ada peringkat
- Survival (Life Table)Dokumen6 halamanSurvival (Life Table)Riyadhi Pasca SyahputraBelum ada peringkat
- Steps and Tools in A Typical Quantitative AnalysisDokumen5 halamanSteps and Tools in A Typical Quantitative Analysisjay cBelum ada peringkat
- Professional Studies PDFDokumen132 halamanProfessional Studies PDFRutendo TaperaBelum ada peringkat
- Qualitative Research Methods: Winston Jackson and Norine VerbergDokumen54 halamanQualitative Research Methods: Winston Jackson and Norine VerbergDilshad ShahBelum ada peringkat
- Definition of ResearchDokumen8 halamanDefinition of ResearchsuparswachakrabortyBelum ada peringkat
- The Informal Constitution - Abhinav ChandrachudDokumen317 halamanThe Informal Constitution - Abhinav ChandrachudRaoBelum ada peringkat
- CHAPTER 2 Marketing ManagementDokumen8 halamanCHAPTER 2 Marketing ManagementRuby De GranoBelum ada peringkat
- Practical Research 2 Budget Plan 2019-2020Dokumen3 halamanPractical Research 2 Budget Plan 2019-2020Rex LimBelum ada peringkat
- qt73h7k69k PDFDokumen13 halamanqt73h7k69k PDFSyukriansah SyukurBelum ada peringkat
- Analysing The Characteristics and Performance of Islamic FundsDokumen387 halamanAnalysing The Characteristics and Performance of Islamic FundsIman KushairiBelum ada peringkat
- Benefits of Eteeap FinalDokumen23 halamanBenefits of Eteeap FinalDj22 Jake100% (2)
- Research 1 Midterm ExamDokumen4 halamanResearch 1 Midterm ExamGian QuiñonesBelum ada peringkat
- Mean Median Mode RangeDokumen21 halamanMean Median Mode RangeDippak Chabra100% (2)
- Reliability and Validity in Qualitative ResearchDokumen87 halamanReliability and Validity in Qualitative Researchekchuem100% (3)
- Lesson Plan in Grade 11 Practical Research I I. Objective Differentiates Quantitative From Qualitative Research (II. Subject MatterDokumen3 halamanLesson Plan in Grade 11 Practical Research I I. Objective Differentiates Quantitative From Qualitative Research (II. Subject MatterANNA CLARISSA AVESBelum ada peringkat
- Communication ResearchDokumen172 halamanCommunication ResearchnekusakurabaBelum ada peringkat
- Research Methodology: SR Ts Siti Hafsah BT ZulkarnainDokumen30 halamanResearch Methodology: SR Ts Siti Hafsah BT ZulkarnainNURAIN HANIS BINTI ARIFFBelum ada peringkat
- Improving Reading AchievementDokumen111 halamanImproving Reading AchievementZyra Rose Leachon - YamsuanBelum ada peringkat
- Evidence Based Practice Medication ErrorsDokumen6 halamanEvidence Based Practice Medication Errorsapi-302591810Belum ada peringkat
- Overview About The Internal Assessment: Ib Topic or OptionDokumen8 halamanOverview About The Internal Assessment: Ib Topic or OptionD'Andra WilliamsBelum ada peringkat
- Jeppiaar Engineering College: Department of Management Studies BATCH 2017 - 2019 I Year / Ii SemesterDokumen136 halamanJeppiaar Engineering College: Department of Management Studies BATCH 2017 - 2019 I Year / Ii SemesterPravitha SajeeBelum ada peringkat