Anda mungkin juga menyukai
- 8 Week CCRN Study PlanDokumen6 halaman8 Week CCRN Study PlanJoshua Atienza100% (2)
- Serrapeptase - The Miracle Enzyme Which Can Save Your LifeDokumen53 halamanSerrapeptase - The Miracle Enzyme Which Can Save Your LifeRoger-Peter Weizenegger100% (7)
- The Way You BreatheDokumen48 halamanThe Way You Breathestevens106100% (1)
- CASE PRESENTATION ON. Respiratory DistresssDokumen13 halamanCASE PRESENTATION ON. Respiratory DistresssArchana Sahu78% (9)
- Community Acquired PneumoniaDokumen56 halamanCommunity Acquired Pneumoniashiean06Belum ada peringkat
- 1020 Final EvaluationDokumen9 halaman1020 Final Evaluationapi-456466614Belum ada peringkat
- A Comprehensive Neurological Examination Guide and Approach To LocalizationDokumen86 halamanA Comprehensive Neurological Examination Guide and Approach To LocalizationLiberty AgcaoiliBelum ada peringkat
- Workshop #4 Internal Medicine IDokumen78 halamanWorkshop #4 Internal Medicine Ihevinpatel100% (1)
- I. Understanding The Disease and PathophysiologyDokumen11 halamanI. Understanding The Disease and PathophysiologyFajer AleitanBelum ada peringkat
- Cardiopulmonary 2 2010 Q OnlyDokumen10 halamanCardiopulmonary 2 2010 Q OnlyWenzy CruzBelum ada peringkat
- 'Batangas Medical Center Case Report by PGI Carlos H. AcuñaDokumen7 halaman'Batangas Medical Center Case Report by PGI Carlos H. AcuñaCarlos H. AcuñaBelum ada peringkat
- Alpha-1-Antitrypsin DeficiencyDokumen13 halamanAlpha-1-Antitrypsin DeficiencyMuhammad SaifullohBelum ada peringkat
- CC 4 Nov 2017 SeizureDokumen44 halamanCC 4 Nov 2017 SeizurenisaBelum ada peringkat
- CC 4 Nov 2017 SeizureDokumen44 halamanCC 4 Nov 2017 SeizureLilik NatasubrataBelum ada peringkat
- Copd TTDDokumen29 halamanCopd TTDWolvistaBelum ada peringkat
- Leaflet Gizi Buruk Wi2ngDokumen36 halamanLeaflet Gizi Buruk Wi2ngAngga PahBelum ada peringkat
- CC DBD 12 Nov 2017Dokumen52 halamanCC DBD 12 Nov 2017Irfan Dzakir NugrohoBelum ada peringkat
- Family Case Presentation: Abat FamilyDokumen80 halamanFamily Case Presentation: Abat FamilyGeraldine Marie SalvoBelum ada peringkat
- Pcapreport 140325070411 Phpapp02Dokumen65 halamanPcapreport 140325070411 Phpapp02Anton RossiniBelum ada peringkat
- CC 10 NOv 2017 ITPDokumen32 halamanCC 10 NOv 2017 ITPLilik NatasubrataBelum ada peringkat
- Program Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaDokumen27 halamanProgram Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaIka AyuBelum ada peringkat
- Morning Report Thursday, 4 July 2017Dokumen39 halamanMorning Report Thursday, 4 July 2017delfiaBelum ada peringkat
- AR 26 April Efusi PleuraDokumen18 halamanAR 26 April Efusi PleuraShaastieBelum ada peringkat
- Bronchiectasis Patient Posted For PneumonectomyDokumen33 halamanBronchiectasis Patient Posted For PneumonectomyANKURBelum ada peringkat
- ROSIMO - AUG 2021 NB VomitingDokumen5 halamanROSIMO - AUG 2021 NB VomitingcarlosBelum ada peringkat
- AR 28 April ACKDDokumen17 halamanAR 28 April ACKDShaastieBelum ada peringkat
- Case V Kardiorespi NovaDokumen41 halamanCase V Kardiorespi NovaArifaniBelum ada peringkat
- Prince Sultan Military College For Health SciencesDokumen20 halamanPrince Sultan Military College For Health SciencesmahaBelum ada peringkat
- Case Conference Saturday Morning Shift, MAY 18, 2019Dokumen39 halamanCase Conference Saturday Morning Shift, MAY 18, 2019Aisya FikritamaBelum ada peringkat
- Workshop #4 Internal Medicine IDokumen78 halamanWorkshop #4 Internal Medicine IhevinpatelBelum ada peringkat
- MR 31 Jan 2021 - BronkopneumoniaDokumen30 halamanMR 31 Jan 2021 - Bronkopneumoniagalihrahman51Belum ada peringkat
- AR Kelompok G - ADB+ HemoroidDokumen22 halamanAR Kelompok G - ADB+ HemoroidSagung Ari DipratariBelum ada peringkat
- AR Kelompok G - ADB+ HemoroidDokumen22 halamanAR Kelompok G - ADB+ HemoroidChindy SarindraBelum ada peringkat
- Case Infeksi TetanusDokumen36 halamanCase Infeksi TetanusIndri Ayu PratiwiBelum ada peringkat
- January 9 SGDDokumen7 halamanJanuary 9 SGDRONALDO CUABelum ada peringkat
- CC 17 Feb 2017 1st Epilepsy OkeDokumen43 halamanCC 17 Feb 2017 1st Epilepsy OkeLucky Yoga -satria NatasukmaBelum ada peringkat
- Case Report: Advisor: Dr. Riki Tenggara, SP - Pd-KGEHDokumen33 halamanCase Report: Advisor: Dr. Riki Tenggara, SP - Pd-KGEHVincentiusBelum ada peringkat
- Orning Eport: Reported By: Tita - Siti Moderator: Dr. Suyoso, SP - PD Tuesday, November 27 2018Dokumen14 halamanOrning Eport: Reported By: Tita - Siti Moderator: Dr. Suyoso, SP - PD Tuesday, November 27 2018Tita RetnoBelum ada peringkat
- Case Conference Pneumonia 17-08-19Dokumen43 halamanCase Conference Pneumonia 17-08-19Primadiati Nickyta SariBelum ada peringkat
- CC 18 Mei 19 HidrocephalusDokumen50 halamanCC 18 Mei 19 HidrocephalusAisya FikritamaBelum ada peringkat
- PP CaseDokumen48 halamanPP CaseDany PrabowoBelum ada peringkat
- AGN 3B FinalDokumen37 halamanAGN 3B FinalKristine Dela CruzBelum ada peringkat
- Case Asma TikaDokumen45 halamanCase Asma TikaMainur TikaBelum ada peringkat
- Morning Report Sunday, July 22 2018 Night ShiftDokumen51 halamanMorning Report Sunday, July 22 2018 Night ShiftantogantengbangetzBelum ada peringkat
- Anaesthetic Man-WPS OfficeDokumen21 halamanAnaesthetic Man-WPS OfficeAnuja KumaresonBelum ada peringkat
- CC 2 Mei 2017 PneumoniaDokumen37 halamanCC 2 Mei 2017 PneumoniaAhimsa Yoga AninditaBelum ada peringkat
- Kunwor Bishal Neuro Case 1Dokumen12 halamanKunwor Bishal Neuro Case 1Bishal JB KunworBelum ada peringkat
- Mohammad Hamid Sabibi - 720621465Dokumen11 halamanMohammad Hamid Sabibi - 720621465Farida Trinovita SariBelum ada peringkat
- Rheumatoid Arthritis LapsusDokumen37 halamanRheumatoid Arthritis Lapsusderahmat dedyBelum ada peringkat
- Case AsmaDokumen21 halamanCase AsmabungaamiliasuariBelum ada peringkat
- Hashim Major LogDokumen26 halamanHashim Major LogHashim AlsammawiBelum ada peringkat
- Pediatric History Taking & Pe Simulation: Student'S Task Done Not DoneDokumen8 halamanPediatric History Taking & Pe Simulation: Student'S Task Done Not DoneFrancis CervantesBelum ada peringkat
- Slide Laporan Kasus - MorbiliDokumen22 halamanSlide Laporan Kasus - MorbiliRielz ThereaperzBelum ada peringkat
- Kasus Perdarahan Intrakranial Pada Bayi Baru LahirDokumen58 halamanKasus Perdarahan Intrakranial Pada Bayi Baru LahirSilvia PAgitta TariganBelum ada peringkat
- Case Report DHF FadhilDokumen49 halamanCase Report DHF FadhilPashëm IndonesiaBelum ada peringkat
- Synapse in My Pocket Neuro Exam & Localization - 1st Ed 2020Dokumen63 halamanSynapse in My Pocket Neuro Exam & Localization - 1st Ed 2020SnowyBelum ada peringkat
- Shock SepticDokumen35 halamanShock SepticAkbar SyarialBelum ada peringkat
- Morning Report 30-9Dokumen15 halamanMorning Report 30-9annisa edwarBelum ada peringkat
- Polymyalgia RheumaticaDokumen23 halamanPolymyalgia RheumaticaGabriella TungadiBelum ada peringkat
- Interna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityDokumen46 halamanInterna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityErni JawaBelum ada peringkat
- Salin-CONTOH LAPORAN KASUS PROSES KEPERAWATANDokumen11 halamanSalin-CONTOH LAPORAN KASUS PROSES KEPERAWATANBriantika Aura jolieBelum ada peringkat
- Harisman BosarDokumen15 halamanHarisman BosarHafizahLatifBelum ada peringkat
- Case Conference July 25 2017Dokumen41 halamanCase Conference July 25 2017dhania patraBelum ada peringkat
- CC 13 Juli 2017 MeningoencephalitisDokumen40 halamanCC 13 Juli 2017 MeningoencephalitisdelfiaBelum ada peringkat
- Case Conference Friday Shift, June 30 2017Dokumen49 halamanCase Conference Friday Shift, June 30 2017Izni AyuniBelum ada peringkat
- Bab Ii Status PasienDokumen12 halamanBab Ii Status PasienNita KurniasihBelum ada peringkat
- STATE - EXAM (Internal Disease)Dokumen72 halamanSTATE - EXAM (Internal Disease)yashrajbarfa0002Belum ada peringkat
- COPD NEW GuidelinesDokumen45 halamanCOPD NEW GuidelinesMuhammad HaneefBelum ada peringkat
- Breathing DifficultyDokumen13 halamanBreathing DifficultygivamathanBelum ada peringkat
- 11 Lung PathologyDokumen7 halaman11 Lung PathologycarlgangcaBelum ada peringkat
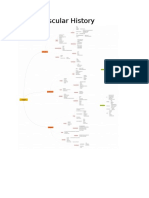
- Cardiovascular History MindmapDokumen12 halamanCardiovascular History MindmapThe_BakerBelum ada peringkat
- A Figure of SpeechDokumen3 halamanA Figure of SpeechRaine del RosarioBelum ada peringkat
- Pulm SIM Outline - MineDokumen4 halamanPulm SIM Outline - MineEvanBelum ada peringkat
- Palliative Care - Overview of Cough, Stridor, and Hemoptysis - UpToDateDokumen19 halamanPalliative Care - Overview of Cough, Stridor, and Hemoptysis - UpToDateThaísa NogueiraBelum ada peringkat
- Case Presentation 1 CopdDokumen48 halamanCase Presentation 1 CopdPreeti ChouhanBelum ada peringkat
- Farmakoterapi PPOK PDFDokumen61 halamanFarmakoterapi PPOK PDFElizabeth SniderBelum ada peringkat
- Impact of Home Mechanical Ventilation On Health-Related Quality of LifeDokumen9 halamanImpact of Home Mechanical Ventilation On Health-Related Quality of LifemartingomezrBelum ada peringkat
- 07.03.09 Chest Physiotherapy PDFDokumen9 halaman07.03.09 Chest Physiotherapy PDFRakesh KumarBelum ada peringkat
- Prosthodontic Management of Geriatric PatientDokumen101 halamanProsthodontic Management of Geriatric PatientMrunal Doiphode100% (2)
- Kasus Farter 2 10 Mei 2019Dokumen3 halamanKasus Farter 2 10 Mei 2019YonicaryanBelum ada peringkat
- Guidelines For The Physiotherapy Management of Chronic Obstructive Pulmonary DiseaseDokumen7 halamanGuidelines For The Physiotherapy Management of Chronic Obstructive Pulmonary DiseaseAyu AryaDewi PasyaViraBelum ada peringkat
- Upper Limb Stretching Terhadap Skala Dispnea Pada Pasien PPOKDokumen7 halamanUpper Limb Stretching Terhadap Skala Dispnea Pada Pasien PPOKrifka riskaBelum ada peringkat
- The Evaluation, Diagnosis, and Treatment of The Adult Patient With Acute Hypercapnic Respiratory Failure - UpToDateDokumen37 halamanThe Evaluation, Diagnosis, and Treatment of The Adult Patient With Acute Hypercapnic Respiratory Failure - UpToDateKiran AsrannaBelum ada peringkat
- Ill Effects of Air Water and Noise PollutionDokumen13 halamanIll Effects of Air Water and Noise PollutionnatashaBelum ada peringkat
- Industry Use Cases - TNASDCDokumen13 halamanIndustry Use Cases - TNASDCAnbarasu anbarasuBelum ada peringkat
- Maintenance of Urban TransportDokumen4 halamanMaintenance of Urban TransportrscordovaBelum ada peringkat
- Mechanism of Breath Sounds ProductionDokumen10 halamanMechanism of Breath Sounds ProductionMonica_azizaBelum ada peringkat
- Alternative Carriers in Dry Powder InhalerDokumen9 halamanAlternative Carriers in Dry Powder InhalerApoorva KBelum ada peringkat
- Examination of Respiratory SystemDokumen78 halamanExamination of Respiratory Systemwidya sri hastutiBelum ada peringkat