Anda mungkin juga menyukai
- Non-Selective Cox 1&2 Inhibitors: AspirinDokumen13 halamanNon-Selective Cox 1&2 Inhibitors: AspirinKristijan GoldašićBelum ada peringkat
- Antipyretic-Analgesic and Antiinflammatory DrugsDokumen46 halamanAntipyretic-Analgesic and Antiinflammatory DrugsAYU SUKARNI PUTRIBelum ada peringkat
- Individual Nsaids: Dr. Estabraq MahmoodDokumen4 halamanIndividual Nsaids: Dr. Estabraq MahmoodJsnanbjrihBelum ada peringkat
- Non Steroidal Anti Inflammatory Drugs 72768501 2Dokumen68 halamanNon Steroidal Anti Inflammatory Drugs 72768501 2AnushaBelum ada peringkat
- Anti-Inflammatory Drugs Lec 3 and 4 LatestDokumen37 halamanAnti-Inflammatory Drugs Lec 3 and 4 Latests.nilormee1201Belum ada peringkat
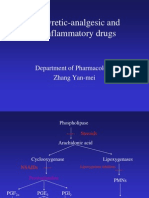
- Antipyretic-Analgesic and Antiinflammatory Drugs: Department of Pharmacology Zhang Yan-MeiDokumen39 halamanAntipyretic-Analgesic and Antiinflammatory Drugs: Department of Pharmacology Zhang Yan-MeiIshu SethiBelum ada peringkat
- NsaidDokumen31 halamanNsaidDr. Hadia NadeemBelum ada peringkat
- Antiplatelets: Prabina - P K 2 ND MSC Nursing Govt. College of Nursing KozhikodeDokumen53 halamanAntiplatelets: Prabina - P K 2 ND MSC Nursing Govt. College of Nursing Kozhikodeanju rachel joseBelum ada peringkat
- DRUGS PediatricsDokumen42 halamanDRUGS PediatricsRAJ BADMERABelum ada peringkat
- Nsaidsacetaminophen 190220064047Dokumen32 halamanNsaidsacetaminophen 190220064047AugustinoBelum ada peringkat
- DR - Hussam Lec 3 Drugs Affecting Blood 2023 4Dokumen13 halamanDR - Hussam Lec 3 Drugs Affecting Blood 2023 4ManWol JangBelum ada peringkat
- Aspirin & NsaidDokumen28 halamanAspirin & NsaidrafiaBelum ada peringkat
- Nonsteroidal Antiinflammatory Drugs and Antipyretic-AnalgesicsDokumen49 halamanNonsteroidal Antiinflammatory Drugs and Antipyretic-AnalgesicsShivsharanBelum ada peringkat
- TDM of SalicylateDokumen23 halamanTDM of Salicylatemingyu safinaBelum ada peringkat
- Anti Inflamatory Drugs AINSDokumen39 halamanAnti Inflamatory Drugs AINSEl FaroukBelum ada peringkat
- NsaidDokumen51 halamanNsaidDebasis Sahoo100% (1)
- Tatalaksana Hiponatremia, Hiperkalemia, HipomagnesiemiaDokumen15 halamanTatalaksana Hiponatremia, Hiperkalemia, HipomagnesiemiaUdyani AgustinaBelum ada peringkat
- Cholinergic Agonist: (Direct Acting)Dokumen31 halamanCholinergic Agonist: (Direct Acting)Shaukat HayatBelum ada peringkat
- Discovery of Aspirin: Presented By: Group 5Dokumen42 halamanDiscovery of Aspirin: Presented By: Group 5LimYiBelum ada peringkat
- 8238412-Gout PharmacologyDokumen28 halaman8238412-Gout Pharmacologyabdomatook272Belum ada peringkat
- Obat Emergensi Dalam AnestesiDokumen32 halamanObat Emergensi Dalam AnestesiNaja NugrahaBelum ada peringkat
- Anti Pyretic 2013Dokumen15 halamanAnti Pyretic 2013Faizah Al GhamdiBelum ada peringkat
- Drugs Used in CcuDokumen169 halamanDrugs Used in CcuAnusha Verghese100% (3)
- PAIN ControllersDokumen39 halamanPAIN ControllersAyro Business CenterBelum ada peringkat
- Anti-Gout DrugsDokumen23 halamanAnti-Gout DrugsphetotzBelum ada peringkat
- Antiplateletdrugs 150203231404 Conversion Gate01 PDFDokumen67 halamanAntiplateletdrugs 150203231404 Conversion Gate01 PDFAndrie WigunaBelum ada peringkat
- Materi 7 - Gagal Ginjal AkutDokumen30 halamanMateri 7 - Gagal Ginjal AkutTegar Muhamad RifkiBelum ada peringkat
- Nonsteroidal Anti-Inflammatory Drugs NSAIDs-2Dokumen25 halamanNonsteroidal Anti-Inflammatory Drugs NSAIDs-2VibeBelum ada peringkat
- Medical Treatment For MiDokumen35 halamanMedical Treatment For MiFev BanataoBelum ada peringkat
- NSAIDsDokumen114 halamanNSAIDsMani Jee100% (1)
- Poisoning: PWM Olly Indrajani 2014Dokumen45 halamanPoisoning: PWM Olly Indrajani 2014arieska daraBelum ada peringkat
- 9 AntiinflammatoryDokumen21 halaman9 AntiinflammatoryAmr SalemBelum ada peringkat
- Anti Gout: by Dr. Saba TariqDokumen32 halamanAnti Gout: by Dr. Saba TariqDr. Saba TariqBelum ada peringkat
- Drug Induced Kidney DiseasesDokumen34 halamanDrug Induced Kidney DiseasesManhal A AbdulkaderBelum ada peringkat
- Pharmagout 190907102528Dokumen42 halamanPharmagout 190907102528AugustinoBelum ada peringkat
- Antpyretic-Analgesic and Antinlammatory DrugsDokumen38 halamanAntpyretic-Analgesic and Antinlammatory DrugskasondaBelum ada peringkat
- Musculo Psik 2012Dokumen38 halamanMusculo Psik 2012Dianita RetnaniBelum ada peringkat
- Hyperglycemia Crisis: Dr. Netty NurnaningtyasDokumen34 halamanHyperglycemia Crisis: Dr. Netty Nurnaningtyasnetty nurnaningtyasBelum ada peringkat
- Pain and Nsaids: Md. Amran Howlader IUB PharmacyDokumen18 halamanPain and Nsaids: Md. Amran Howlader IUB PharmacySumaya OrnaBelum ada peringkat
- Drugs of CvsDokumen32 halamanDrugs of CvsAgus HaryantoBelum ada peringkat
- NSAIDsDokumen54 halamanNSAIDsAlaaBelum ada peringkat
- Inotropes, Excellent Article, With DosingDokumen47 halamanInotropes, Excellent Article, With DosingNavojit ChowdhuryBelum ada peringkat
- Antigout PDFDokumen21 halamanAntigout PDFshaifBelum ada peringkat
- Antiplatelete DrugsDokumen27 halamanAntiplatelete DrugsYohannes MeridBelum ada peringkat
- TabletsDokumen6 halamanTabletsRupesh Kumar DuttaBelum ada peringkat
- Management of Potassium Disorders 17706 ArticleDokumen4 halamanManagement of Potassium Disorders 17706 ArticlealeBelum ada peringkat
- 8 Drug StudyDokumen19 halaman8 Drug StudyLoyloy D ManBelum ada peringkat
- Mefenamic Acid Indication, Dosage, Side Effect, Precaution MIMS MalaysiaDokumen1 halamanMefenamic Acid Indication, Dosage, Side Effect, Precaution MIMS MalaysianuruladyanisaifuzzamanBelum ada peringkat
- Introduction CarbamazepineDokumen4 halamanIntroduction Carbamazepineammaramaryam6463Belum ada peringkat
- SAQ - NSAIDS Mechanism and Side Effect 180209Dokumen6 halamanSAQ - NSAIDS Mechanism and Side Effect 180209anaeshkl100% (1)
- Product Monograph: (Acetylsalicylic Acid Chewable Tablets, USP) 81 MGDokumen31 halamanProduct Monograph: (Acetylsalicylic Acid Chewable Tablets, USP) 81 MGعبدالعزيز بدرBelum ada peringkat
- NSAIDsDokumen27 halamanNSAIDsshatz_014Belum ada peringkat
- Acetylsalicylic Acid (Aspirin) : PharmachologyDokumen11 halamanAcetylsalicylic Acid (Aspirin) : PharmachologywawaBelum ada peringkat
- HyperkalaemiaDokumen6 halamanHyperkalaemiaSSBelum ada peringkat
- Acetylsalicylic Acid (Aspirin) : 1190159 3 GradeDokumen8 halamanAcetylsalicylic Acid (Aspirin) : 1190159 3 GradeAbdelrhman AboodaBelum ada peringkat
- Case 1 & 2Dokumen4 halamanCase 1 & 2Adeel ShahidBelum ada peringkat
- Cholinomimetic DrugsDokumen33 halamanCholinomimetic DrugsMarsh MelloBelum ada peringkat
- AH PharmaII v2Dokumen35 halamanAH PharmaII v2bankai2992Belum ada peringkat
- PharmaDokumen8 halamanPharma2022105340Belum ada peringkat
- GARDNERELLADokumen15 halamanGARDNERELLADesti Ratna PutriBelum ada peringkat
- Haemophilus DucreyiDokumen15 halamanHaemophilus DucreyiDesti Ratna Putri100% (1)
- Metabolic Syndrome: Arsiniati M.Brata - ArbaiDokumen21 halamanMetabolic Syndrome: Arsiniati M.Brata - ArbaiDesti Ratna PutriBelum ada peringkat
- Coronary Artery Disease: Dr. Sadewantoro, SP - JP, FIHA Fakultas Kedokteran Universitas Hang TuahDokumen76 halamanCoronary Artery Disease: Dr. Sadewantoro, SP - JP, FIHA Fakultas Kedokteran Universitas Hang TuahDesti Ratna PutriBelum ada peringkat
- Antihypertension: Prajogo WibowoDokumen45 halamanAntihypertension: Prajogo WibowoDesti Ratna PutriBelum ada peringkat
- Kuliah Sem 4 '13 THX Intervensi KVDokumen39 halamanKuliah Sem 4 '13 THX Intervensi KVDesti Ratna PutriBelum ada peringkat
- VRF-SLB013-EN - 0805115 - Catalogo Ingles 2015 PDFDokumen50 halamanVRF-SLB013-EN - 0805115 - Catalogo Ingles 2015 PDFJhon Lewis PinoBelum ada peringkat
- Module 11 Activity Based CostingDokumen13 halamanModule 11 Activity Based CostingMarjorie NepomucenoBelum ada peringkat
- Volcanic SoilsDokumen14 halamanVolcanic SoilsVictor Hugo BarbosaBelum ada peringkat
- AnnexIIRecommendationsbyHOTCCommittee06 11 18Dokumen6 halamanAnnexIIRecommendationsbyHOTCCommittee06 11 18Bilal AbbasBelum ada peringkat
- Complete DaikinDokumen11 halamanComplete DaikinAGNIDEEP BAIDYABelum ada peringkat
- MINDSET 1 EXERCISES TEST 1 Pendientes 1º Bach VOCABULARY AND GRAMMARDokumen7 halamanMINDSET 1 EXERCISES TEST 1 Pendientes 1º Bach VOCABULARY AND GRAMMARanaBelum ada peringkat
- Soal PTS Vii BigDokumen6 halamanSoal PTS Vii Bigdimas awe100% (1)
- Language Loss in Waray: Ni Voltaire Q. UyzonDokumen23 halamanLanguage Loss in Waray: Ni Voltaire Q. UyzonMary Rose OmbrogBelum ada peringkat
- Arabian Choice General Trading Co. LLCDokumen1 halamanArabian Choice General Trading Co. LLCjaanBelum ada peringkat
- RG-RAP6260 (G) Hardware InstallationDokumen26 halamanRG-RAP6260 (G) Hardware InstallationrazuetBelum ada peringkat
- Dr. N. Kumarappan IE (I) Council Candidate - Electrical DivisionDokumen1 halamanDr. N. Kumarappan IE (I) Council Candidate - Electrical Divisionshanmugasundaram32Belum ada peringkat
- IAU Logbook Core 6weeksDokumen7 halamanIAU Logbook Core 6weeksbajariaaBelum ada peringkat
- Environmental and Chemical Policy Module3Dokumen47 halamanEnvironmental and Chemical Policy Module3jahazi1Belum ada peringkat
- T HR El 20003 ST PDFDokumen20 halamanT HR El 20003 ST PDFAngling Dharma100% (1)
- Firststep To AlaskaDokumen28 halamanFirststep To AlaskaBarbara NelsonBelum ada peringkat
- A Technical Report ON Centre of Pressure ONA Plane Surface ExperimentDokumen13 halamanA Technical Report ON Centre of Pressure ONA Plane Surface ExperimentVictor OwolekeBelum ada peringkat
- Pamphlet On Arrangement of Springs in Various Casnub Trolleys Fitted On Air Brake Wagon PDFDokumen9 halamanPamphlet On Arrangement of Springs in Various Casnub Trolleys Fitted On Air Brake Wagon PDFNiKhil GuPtaBelum ada peringkat
- 5024Dokumen2 halaman5024Luis JesusBelum ada peringkat
- Solutions For Tutorial Exercises Association Rule Mining.: Exercise 1. AprioriDokumen5 halamanSolutions For Tutorial Exercises Association Rule Mining.: Exercise 1. AprioriMarkib Singh AdawitahkBelum ada peringkat
- Equipment Maintenance and Measuring Equipment ProcedureDokumen2 halamanEquipment Maintenance and Measuring Equipment ProcedureRaja Mani100% (1)
- Instructional Decision MakingDokumen5 halamanInstructional Decision Makingapi-257693907Belum ada peringkat
- ISA Guidelines PPF 1Dokumen19 halamanISA Guidelines PPF 1Vasu DevanBelum ada peringkat
- AA1 Adventure Anthology One r14Dokumen85 halamanAA1 Adventure Anthology One r14dachda100% (1)
- Unit 4 ADokumen10 halamanUnit 4 AChetan p ShirahattiBelum ada peringkat
- Organic Food Business in India A Survey of CompaniDokumen19 halamanOrganic Food Business in India A Survey of CompaniShravan KemturBelum ada peringkat
- Ageing World ReportDokumen4 halamanAgeing World Reporttheresia anggitaBelum ada peringkat
- LEARNING ACTIVITY SHEET in Oral CommDokumen4 halamanLEARNING ACTIVITY SHEET in Oral CommTinTin100% (1)
- Atlantis Implant Compatibility Chart 79214-US-1107Dokumen2 halamanAtlantis Implant Compatibility Chart 79214-US-1107Jean-Christophe PopeBelum ada peringkat
- Safe Motherhood Ao2016-0035 Quality Antenatal Care PDFDokumen9 halamanSafe Motherhood Ao2016-0035 Quality Antenatal Care PDFGa B B OrlonganBelum ada peringkat
- Revised LabDokumen18 halamanRevised LabAbu AyemanBelum ada peringkat