Anda mungkin juga menyukai
- The Blockbuster Drugs Outlook PDFDokumen259 halamanThe Blockbuster Drugs Outlook PDFHerry HendrayadiBelum ada peringkat
- MRCP revision: commonly tested facts about causes, treatments and prognosesDokumen6 halamanMRCP revision: commonly tested facts about causes, treatments and prognosesMohamed Amr SalamaBelum ada peringkat
- Bovine Common Diagnosis Review For NAVLE.Dokumen46 halamanBovine Common Diagnosis Review For NAVLE.Mayank Mj Patel100% (2)
- MKSAP NotesDokumen31 halamanMKSAP NotesJared MasonBelum ada peringkat
- 05 - Sle, DMZ, PHSDokumen157 halaman05 - Sle, DMZ, PHSG SBelum ada peringkat
- Pinggang PinoyDokumen9 halamanPinggang Pinoyjreyab100% (1)
- Benefits of Spa Treatment Types of Spa TreatmentDokumen6 halamanBenefits of Spa Treatment Types of Spa TreatmentCris Cali EspeBelum ada peringkat
- Lupus Nephritis1Dokumen45 halamanLupus Nephritis1Lingga GumelarBelum ada peringkat
- Critical Incident Stress Debriefing GuideDokumen11 halamanCritical Incident Stress Debriefing GuideMae Goñez100% (2)
- Acute CNS Infections Diagnosis GuideDokumen53 halamanAcute CNS Infections Diagnosis GuideEhab KhiryBelum ada peringkat
- Small PoxDokumen8 halamanSmall PoxDiazBelum ada peringkat
- Morning Report: Jawaria K. Alam, MD/PGY3Dokumen20 halamanMorning Report: Jawaria K. Alam, MD/PGY3Emily EresumaBelum ada peringkat
- Pharma 2020 PWC ReportDokumen32 halamanPharma 2020 PWC ReportBrand SynapseBelum ada peringkat
- Presented By: Dr. Hirdesh Chawla Junior Resident IiiDokumen79 halamanPresented By: Dr. Hirdesh Chawla Junior Resident IiiAzizan HannyBelum ada peringkat
- SLE Concept MapDokumen1 halamanSLE Concept Mapadrienne cervantesBelum ada peringkat
- Autoimmune Disease in ChildrenDokumen41 halamanAutoimmune Disease in ChildrenAulya ArchuletaBelum ada peringkat
- El Exprime Hombres 2Dokumen11 halamanEl Exprime Hombres 2Carlos GonzalezBelum ada peringkat
- Rheumatology Notes For ReadingDokumen8 halamanRheumatology Notes For ReadingMohamed Rikarz Ahamed RikarzBelum ada peringkat
- 12.2.09 Crocker SLEDokumen24 halaman12.2.09 Crocker SLENununNur'aeniMusthofaBelum ada peringkat
- Systemic Lupus Erythematosus - An Overview: - Dr. Parvez KhanDokumen68 halamanSystemic Lupus Erythematosus - An Overview: - Dr. Parvez KhanMohammad Sadiq AzamBelum ada peringkat
- DR - Nadrizal - Sle Dan RaDokumen24 halamanDR - Nadrizal - Sle Dan RaPutri Sari SeptirianiBelum ada peringkat
- Portofolio SHDokumen22 halamanPortofolio SHDini Jatiya AnggrainiBelum ada peringkat
- Diagnosing and Managing Systemic Lupus ErythematosusDokumen3 halamanDiagnosing and Managing Systemic Lupus ErythematosusAlya Putri KhairaniBelum ada peringkat
- Mening Enceph Old PatDokumen64 halamanMening Enceph Old PatmutiaBelum ada peringkat
- Fever: &knee PainDokumen49 halamanFever: &knee PainJohn Christopher LucesBelum ada peringkat
- Histiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesDokumen41 halamanHistiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesChetan SekhriBelum ada peringkat
- LES Mar Cad OresDokumen4 halamanLES Mar Cad OresAlberto StrusbergBelum ada peringkat
- Lupus ErythematosusDokumen5 halamanLupus ErythematosusAditya DarmawanBelum ada peringkat
- SleDokumen33 halamanSleZaira HussainBelum ada peringkat
- Cornell Notes: TopicDokumen4 halamanCornell Notes: TopicLeahCongrehillaBelum ada peringkat
- Lymphoma: 2011-2012 Prof - Dr.Rejin Kebudi, M.DDokumen57 halamanLymphoma: 2011-2012 Prof - Dr.Rejin Kebudi, M.Dmia rachmiBelum ada peringkat
- SLE-combined 2 ArshadDokumen71 halamanSLE-combined 2 ArshadarshadsyahaliBelum ada peringkat
- DR Romila Chimoriya Lecturer Department of Pediatrics: Acute Rheumatic FeverDokumen27 halamanDR Romila Chimoriya Lecturer Department of Pediatrics: Acute Rheumatic FeverDhiraj PantBelum ada peringkat
- EncephalitisDokumen30 halamanEncephalitisHITIPHYSIO100% (1)
- Meningitis Beyond The Neonatal AgeDokumen51 halamanMeningitis Beyond The Neonatal AgeBeamlak Getachew WoldeselassieBelum ada peringkat
- Hand Out SJS TEN - 201104Dokumen48 halamanHand Out SJS TEN - 201104Duke ChungBelum ada peringkat
- Acquired Heart Disease in PediatricsDokumen130 halamanAcquired Heart Disease in Pediatricsณัช เกษมBelum ada peringkat
- Anesthesia For Systemic Lupus Erythematosus ReviewDokumen12 halamanAnesthesia For Systemic Lupus Erythematosus ReviewAnonymous x75qV3lGBelum ada peringkat
- DR - Farhad Salehzadeh Connective Tissue DiseaseDokumen70 halamanDR - Farhad Salehzadeh Connective Tissue DiseaseLinux LinuxBelum ada peringkat
- Systemic Lupus Erythematosus: Harrison's ClubDokumen60 halamanSystemic Lupus Erythematosus: Harrison's ClubOrchid Limoso LozanoBelum ada peringkat
- Systemic Lupus Erythematosus (SLE)Dokumen13 halamanSystemic Lupus Erythematosus (SLE)Kathrina IoannouBelum ada peringkat
- SleDokumen26 halamanSleChikezie OnwukweBelum ada peringkat
- Understanding Leukaemia: Causes, Diagnosis and TreatmentDokumen64 halamanUnderstanding Leukaemia: Causes, Diagnosis and TreatmentAnastasiafynnBelum ada peringkat
- Department of Neurology-Padjadjaran University-Bandung: Nushrotul Lailiyya M.DDokumen35 halamanDepartment of Neurology-Padjadjaran University-Bandung: Nushrotul Lailiyya M.DeuiskurBelum ada peringkat
- Meningitis and Encephalitis: Samantha Noll June 11, 2015Dokumen45 halamanMeningitis and Encephalitis: Samantha Noll June 11, 2015galihBelum ada peringkat
- Paediatrics MCQ PointsDokumen117 halamanPaediatrics MCQ PointstharikaneelawathuraBelum ada peringkat
- Nephrotic SyndromeDokumen67 halamanNephrotic SyndromeSharaf EskafiBelum ada peringkat
- Lecture INST-100294 2023 12 08 22 26 10Dokumen62 halamanLecture INST-100294 2023 12 08 22 26 10Pughal PrabakarBelum ada peringkat
- Morning Report: Aaron Mccoy, MD, Pgy3Dokumen16 halamanMorning Report: Aaron Mccoy, MD, Pgy3Emily EresumaBelum ada peringkat
- Connective Tissue Disorders: Systemic Lupus Erythematosus, Systemic Sclerosis, Antiphospholipid SyndromeDokumen51 halamanConnective Tissue Disorders: Systemic Lupus Erythematosus, Systemic Sclerosis, Antiphospholipid SyndromeKathleenZunigaBelum ada peringkat
- NeurosepsisDokumen29 halamanNeurosepsisRed DevilBelum ada peringkat
- Systemic Lupus Erythematosus (SLE)Dokumen31 halamanSystemic Lupus Erythematosus (SLE)FathimathBelum ada peringkat
- SLE Clinical PatternsDokumen28 halamanSLE Clinical PatternsLuiz Fernando Alves FerreiraBelum ada peringkat
- Non Malignant WBCDokumen12 halamanNon Malignant WBCPALATTAO, AUBRIE L. BSMT2-8Belum ada peringkat
- Systemic Lupus Erythematosus (SLE) Pathogenesis and Diagnostic CriteriaDokumen96 halamanSystemic Lupus Erythematosus (SLE) Pathogenesis and Diagnostic CriteriaDon CaprettoBelum ada peringkat
- Arterial ThrombosisrheumroundsDokumen49 halamanArterial ThrombosisrheumroundsBiniyam AsratBelum ada peringkat
- DR Is - Systemic Lupus ErythematosusDokumen27 halamanDR Is - Systemic Lupus ErythematosusRizky SudarmaBelum ada peringkat
- Referat SLEDokumen24 halamanReferat SLENihayatulHusniaBelum ada peringkat
- Staphylococcal Toxic Shock Syndrome: M Kare, A DangDokumen3 halamanStaphylococcal Toxic Shock Syndrome: M Kare, A DangAnonymous ALlIo2LBelum ada peringkat
- Farmakoterapi - SLEDokumen28 halamanFarmakoterapi - SLEWidi Alya ZhafiraBelum ada peringkat
- Systemic Lupus Erythematosus SLE: DefinitionDokumen19 halamanSystemic Lupus Erythematosus SLE: DefinitionShimmering MoonBelum ada peringkat
- Misc in ChildrenDokumen23 halamanMisc in ChildrenKushalaniBelum ada peringkat
- Acute Lymphoblastic Leukemia Treatment OverviewDokumen22 halamanAcute Lymphoblastic Leukemia Treatment OverviewnoviBelum ada peringkat
- Group A Streptococcal Infections: PatophysiologyDokumen11 halamanGroup A Streptococcal Infections: Patophysiologyrahma perwitasariBelum ada peringkat
- 10.27.06 Cox Aplastic AnemiaDokumen15 halaman10.27.06 Cox Aplastic Anemiaravi2kanthBelum ada peringkat
- Rheumatology SlidesDokumen43 halamanRheumatology Slidesdrmalsharrakhi_32794Belum ada peringkat
- Systemic Lupus ErythematosusDokumen10 halamanSystemic Lupus ErythematosuszkxxyyBelum ada peringkat
- Astellas Pharma: Launches Irribow OD Tablets in Japan For Diarrhea-Predominant Irritable Bowel SyndromeDokumen3 halamanAstellas Pharma: Launches Irribow OD Tablets in Japan For Diarrhea-Predominant Irritable Bowel SyndromeHerry HendrayadiBelum ada peringkat
- BCP 13010 PDFDokumen11 halamanBCP 13010 PDFHerry HendrayadiBelum ada peringkat
- Practical Guide To Joint and Soft Tissue Injection TechniquesDokumen5 halamanPractical Guide To Joint and Soft Tissue Injection TechniquesHerry HendrayadiBelum ada peringkat
- Kharkov National Medical University Department of Pharmacology Lecture on Anti-inflammatory DrugsDokumen82 halamanKharkov National Medical University Department of Pharmacology Lecture on Anti-inflammatory DrugsHerry HendrayadiBelum ada peringkat
- 1 - Dr. KungDokumen18 halaman1 - Dr. KungWawan IndrawanBelum ada peringkat
- Growth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsDokumen176 halamanGrowth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsHerry HendrayadiBelum ada peringkat
- The Top 10 Generic Pharmaceutical CompaniesDokumen42 halamanThe Top 10 Generic Pharmaceutical CompaniesHerry HendrayadiBelum ada peringkat
- The Top 10 Generic Pharmaceutical CompaniesDokumen10 halamanThe Top 10 Generic Pharmaceutical CompaniesHerry HendrayadiBelum ada peringkat
- Standard Step-Wise Timelines in The Drug Discovery ProcessDokumen19 halamanStandard Step-Wise Timelines in The Drug Discovery ProcessHerry HendrayadiBelum ada peringkat
- Press Conference: Astellas' Growth StrategyDokumen31 halamanPress Conference: Astellas' Growth StrategyHerry HendrayadiBelum ada peringkat
- Lifecycle Management Strategies Maximizing ROI Through Indication Expansion Reformulation and Rx-To-OTC SwitchingDokumen176 halamanLifecycle Management Strategies Maximizing ROI Through Indication Expansion Reformulation and Rx-To-OTC SwitchingHerry Hendrayadi100% (1)
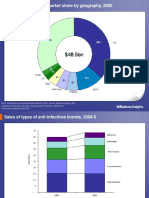
- The Global AntiInfectives Market OutlookDokumen267 halamanThe Global AntiInfectives Market OutlookHerry HendrayadiBelum ada peringkat
- Standard Step-Wise Timelines in The Drug Discovery ProcessDokumen19 halamanStandard Step-Wise Timelines in The Drug Discovery ProcessHerry HendrayadiBelum ada peringkat
- Top 10 Generic Pharmaceutical CompaniesDokumen178 halamanTop 10 Generic Pharmaceutical CompaniesHerry HendrayadiBelum ada peringkat
- The Top 10 Generic Pharmaceutical CompaniesDokumen42 halamanThe Top 10 Generic Pharmaceutical CompaniesHerry HendrayadiBelum ada peringkat
- Pharmaceutical Growth Opportunities in Brazil, Russia, India and ChinaDokumen35 halamanPharmaceutical Growth Opportunities in Brazil, Russia, India and ChinaHerry HendrayadiBelum ada peringkat
- The Global AntiInfectives Market OutlookDokumen267 halamanThe Global AntiInfectives Market OutlookHerry HendrayadiBelum ada peringkat
- Achieving Market Dominance Through Reformulation.Dokumen12 halamanAchieving Market Dominance Through Reformulation.Herry HendrayadiBelum ada peringkat
- Global Market AnalysisaAntibioticsDokumen23 halamanGlobal Market AnalysisaAntibioticsHerry HendrayadiBelum ada peringkat
- Management Pocketbooks - The Balance Sheet PocketbookDokumen309 halamanManagement Pocketbooks - The Balance Sheet PocketbookHerry Hendrayadi100% (1)
- Reader's Digest January 2013Dokumen148 halamanReader's Digest January 2013pereira_jus3430Belum ada peringkat
- Indication Expansion Opportunities For Successful Lifecycle ManagementDokumen144 halamanIndication Expansion Opportunities For Successful Lifecycle ManagementHerry HendrayadiBelum ada peringkat
- Achieving Market Dominance Through ReformulationDokumen223 halamanAchieving Market Dominance Through ReformulationHerry HendrayadiBelum ada peringkat
- Top 15 Therapeutic 2008 PDFDokumen95 halamanTop 15 Therapeutic 2008 PDFHerry HendrayadiBelum ada peringkat
- Growth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsDokumen176 halamanGrowth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsHerry HendrayadiBelum ada peringkat
- 2nd Announcement A5 Upload 1Dokumen18 halaman2nd Announcement A5 Upload 1Herry HendrayadiBelum ada peringkat
- Ijss Aug Oa12Dokumen5 halamanIjss Aug Oa12Herry HendrayadiBelum ada peringkat
- Evidence Map of Cupping Therapy: Clinical MedicineDokumen13 halamanEvidence Map of Cupping Therapy: Clinical MedicineBence KlusóczkiBelum ada peringkat
- Design of An Ergonomic Chair With Headrest and Armrest Using Anthropometric DataDokumen12 halamanDesign of An Ergonomic Chair With Headrest and Armrest Using Anthropometric DatasalehBelum ada peringkat
- The Power of Mental Toughness Building The Foundation For SuccessDokumen129 halamanThe Power of Mental Toughness Building The Foundation For Successcontact.iptvviewBelum ada peringkat
- Final Draft - Sleep EssayDokumen11 halamanFinal Draft - Sleep Essayapi-609533757Belum ada peringkat
- IE PEEPValve 493480001 V03 0413 PDFDokumen2 halamanIE PEEPValve 493480001 V03 0413 PDFCoffee ĐenBelum ada peringkat
- JSA Erection of Steel StructureDokumen9 halamanJSA Erection of Steel StructureOvais FarooqBelum ada peringkat
- SHENAAZ Surgical Chronicles - Final VersionDokumen6 halamanSHENAAZ Surgical Chronicles - Final VersionSumayyah EbrahimBelum ada peringkat
- Performence Appraisal For PracticeDokumen18 halamanPerformence Appraisal For PracticeAnusha VergheseBelum ada peringkat
- 10 Rights in Drug AdministrationDokumen25 halaman10 Rights in Drug AdministrationNathaniel PulidoBelum ada peringkat
- V IMP Chandrika NadiDokumen1.622 halamanV IMP Chandrika NadihcbbBelum ada peringkat
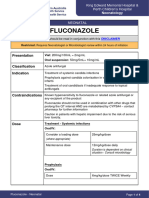
- FluconazoleDokumen4 halamanFluconazoleeucaBelum ada peringkat
- Everything Can Cause Stress: Big Events, Daily Hassles & Life ChangesDokumen4 halamanEverything Can Cause Stress: Big Events, Daily Hassles & Life ChangesOkello StevenBelum ada peringkat
- Chapter Iii KLS 8 SMT IDokumen3 halamanChapter Iii KLS 8 SMT IRizqi Rahmadani Zuhri SaputriBelum ada peringkat
- Contoh CVDokumen1 halamanContoh CVRizki Yulisetiawan100% (1)
- Smartman Flyer 2020Dokumen8 halamanSmartman Flyer 2020Kian GonzagaBelum ada peringkat
- Irc CVDokumen4 halamanIrc CVEmbay AmareBelum ada peringkat
- NASA 162514main Human NeedsDokumen17 halamanNASA 162514main Human NeedsNASAdocuments100% (1)
- Microplastic Communities in Different Environments Differenc - 2021 - Water R PDFDokumen11 halamanMicroplastic Communities in Different Environments Differenc - 2021 - Water R PDFSunita ChayalBelum ada peringkat
- Parcare Assessment MaxillofacialDokumen22 halamanParcare Assessment Maxillofacialqta omerBelum ada peringkat
- Honey and Skin Care Favouriteskmbkj PDFDokumen1 halamanHoney and Skin Care Favouriteskmbkj PDFPritchardBossen37Belum ada peringkat
- LEEP System 1000 Directions For UseeDokumen24 halamanLEEP System 1000 Directions For UseeFernando CosciaBelum ada peringkat
- Chapter 47Dokumen11 halamanChapter 47Aziil LiizaBelum ada peringkat
- Indian Psychology by MadhuDokumen3 halamanIndian Psychology by MadhuSmita DasBelum ada peringkat
- Handtool Safety Training Electric Hand Drill 1. Training Safety PrerequisitesDokumen3 halamanHandtool Safety Training Electric Hand Drill 1. Training Safety Prerequisitesretheep0% (1)