Anda mungkin juga menyukai
- Reproduction System 1Dokumen48 halamanReproduction System 1SITI AISYAHBelum ada peringkat
- Ultrasonography in Pregnancy: Clinical Management Guidelines For Obstetrician-Gynecologists Number 58, December 2004Dokumen30 halamanUltrasonography in Pregnancy: Clinical Management Guidelines For Obstetrician-Gynecologists Number 58, December 2004KamenriderBelum ada peringkat
- Emergency UltrasoundDokumen164 halamanEmergency UltrasoundRamkumar SubburajBelum ada peringkat
- The Role of Ultrasound in Obstetric and Gynaecology: Max Brinsmead PHD Franzcog May 2006Dokumen9 halamanThe Role of Ultrasound in Obstetric and Gynaecology: Max Brinsmead PHD Franzcog May 2006alhassanmohamedBelum ada peringkat
- Time Imaging .: Ultrasonography Machine For Veterinary ApplicationDokumen22 halamanTime Imaging .: Ultrasonography Machine For Veterinary ApplicationKanhaiyalal RamBelum ada peringkat
- Questions From Last Lecture ?: Is It RightDokumen39 halamanQuestions From Last Lecture ?: Is It RightPirin Pin PinBelum ada peringkat
- UTZDokumen12 halamanUTZIyah Bu-ucanBelum ada peringkat
- Ultrasonic Anatomy and Pathology of The Equine UteDokumen13 halamanUltrasonic Anatomy and Pathology of The Equine UteSamantha Orozco PinedaBelum ada peringkat
- Ultrasonic Anatomy and Pathology of The Equine UteDokumen13 halamanUltrasonic Anatomy and Pathology of The Equine UteSamantha Orozco PinedaBelum ada peringkat
- Ectopic 2Dokumen48 halamanEctopic 2Norsri WahyuBelum ada peringkat
- Recent Advances in Pregnancy Diagnosis of Dairy AnimalsDokumen45 halamanRecent Advances in Pregnancy Diagnosis of Dairy AnimalsPratik Wankhade50% (2)
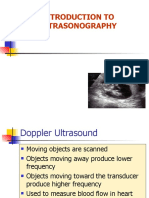
- Introduction To UltrasonographyDokumen44 halamanIntroduction To UltrasonographyPirin Pin PinBelum ada peringkat
- Ultrasonic Assessment of Infertility: Ikuko HondaDokumen8 halamanUltrasonic Assessment of Infertility: Ikuko HondajawaralopangBelum ada peringkat
- DR Ogunwale A.N Ufm UnitDokumen37 halamanDR Ogunwale A.N Ufm UnitzumarockBelum ada peringkat
- View AttachmentDokumen2 halamanView AttachmentkingkhanpfcodBelum ada peringkat
- 2nd Bovine UltrasonographyDokumen72 halaman2nd Bovine UltrasonographyUsama RajpootBelum ada peringkat
- Vaginoscopy and Ultrasonography For Diagnosing Endometritis and Its Therapeutic Management in Repeat Breeder CowsDokumen5 halamanVaginoscopy and Ultrasonography For Diagnosing Endometritis and Its Therapeutic Management in Repeat Breeder CowsGovind Narayan PurohitBelum ada peringkat
- Chronic Ovarian Ectopic Pregnancy - An Unusual Occurrence: A Case ReportDokumen5 halamanChronic Ovarian Ectopic Pregnancy - An Unusual Occurrence: A Case Reportindex PubBelum ada peringkat
- Usg Blok 17Dokumen104 halamanUsg Blok 17iqiqiqiqiqBelum ada peringkat
- 12.10 Sonographic Characteristics of Adnexal TorsionDokumen12 halaman12.10 Sonographic Characteristics of Adnexal Torsionannisha rizkyBelum ada peringkat
- General Introduction of Obstetric UltrasonographyDokumen25 halamanGeneral Introduction of Obstetric Ultrasonographymuhammad alqoriBelum ada peringkat
- First-Trimester Determination of Fetal Gender PDFDokumen3 halamanFirst-Trimester Determination of Fetal Gender PDFkukadiyaBelum ada peringkat
- Yulia AFDokumen12 halamanYulia AFIlmiah Program studi ObginBelum ada peringkat
- How to Perform Ultrasonography in EndometriosisDari EverandHow to Perform Ultrasonography in EndometriosisStefano GuerrieroBelum ada peringkat
- 2011 9 PDFDokumen6 halaman2011 9 PDFRamesh Kumar SBelum ada peringkat
- Chan - Et - Al-2017-A Longitudinal Follow-Up of Pelvic Floor BiometryDokumen24 halamanChan - Et - Al-2017-A Longitudinal Follow-Up of Pelvic Floor BiometryVitalidad PelvicaBelum ada peringkat
- Ultrasound - A GuideDokumen9 halamanUltrasound - A GuideDebasish KunduBelum ada peringkat
- First-Trimester UltrasoundDokumen24 halamanFirst-Trimester UltrasoundYzavo Scarlleth Gutierrez CamposBelum ada peringkat
- Ultrasound in Gynecology N ObstetricDokumen9 halamanUltrasound in Gynecology N ObstetricKarthik RajvBelum ada peringkat
- Cervicometria e InduccionDokumen7 halamanCervicometria e InduccionIdela VizcainoBelum ada peringkat
- 1 - DR Reem Basic OB ScanningDokumen39 halaman1 - DR Reem Basic OB ScanningSabiha SadatBelum ada peringkat
- 10.1007@s00404 006 0180 9Dokumen4 halaman10.1007@s00404 006 0180 9Bara Tracy LovitaBelum ada peringkat
- P15:Secondandthirdtrimestersi: S. Latella, V. Fenu, P. Ceccarelli, F. Baldinotti, L. Iughetti, A. Volpe, V. MazzaDokumen2 halamanP15:Secondandthirdtrimestersi: S. Latella, V. Fenu, P. Ceccarelli, F. Baldinotti, L. Iughetti, A. Volpe, V. MazzaXlr8zzBelum ada peringkat
- Yolk Sac Shape OutcomeDokumen11 halamanYolk Sac Shape OutcomeSofyan QadriBelum ada peringkat
- Vaginal Touch Versus Transvaginal Ultrasound in The Management of Threatened Preterm Labour at The University Hospital Center of Porto-Novo (Benin)Dokumen9 halamanVaginal Touch Versus Transvaginal Ultrasound in The Management of Threatened Preterm Labour at The University Hospital Center of Porto-Novo (Benin)Bayu Diesfa PuteraBelum ada peringkat
- Ultrasound LectureDokumen17 halamanUltrasound LectureYousif Ahmed DABelum ada peringkat
- Spectrum of Normal Intrauterine Cavity Sonographic Findings After First-Trimester AbortionDokumen5 halamanSpectrum of Normal Intrauterine Cavity Sonographic Findings After First-Trimester AbortionOrchid LandBelum ada peringkat
- Ultrasound in ObstetricsDokumen3 halamanUltrasound in ObstetricsSarita DubeyBelum ada peringkat
- Applications of Diagnostic Ultrasonography in Small Ruminant Reproductive ManagementDokumen3 halamanApplications of Diagnostic Ultrasonography in Small Ruminant Reproductive ManagementAlexander Cañar RomeroBelum ada peringkat
- Primary Abdominal Ectopic Pregnancy: A Case ReportDokumen4 halamanPrimary Abdominal Ectopic Pregnancy: A Case ReportYared TJBelum ada peringkat
- NCM 109 1Dokumen97 halamanNCM 109 1martirezdawncelineBelum ada peringkat
- 0068KJR - KJR 5 39Dokumen8 halaman0068KJR - KJR 5 39Louis HadiyantoBelum ada peringkat
- Diagnostic Tools in ObgynDokumen27 halamanDiagnostic Tools in ObgynHenok Y KebedeBelum ada peringkat
- Final Submited Meningomyelocele101010Dokumen13 halamanFinal Submited Meningomyelocele101010agumasBelum ada peringkat
- Transabdominal Sonography Before Uterine Exploration As A Predictor of Retained Placental FragmentsDokumen5 halamanTransabdominal Sonography Before Uterine Exploration As A Predictor of Retained Placental FragmentsDownloadBelum ada peringkat
- The Normal and Pathologic Postpartum UterusDokumen10 halamanThe Normal and Pathologic Postpartum UterusAlberto BrahmBelum ada peringkat
- The Role Ultrasound in Early PregnancyDokumen167 halamanThe Role Ultrasound in Early PregnancyCordova ArridhoBelum ada peringkat
- Lecture 4. Perinatology As A ScienceDokumen58 halamanLecture 4. Perinatology As A ScienceBabbu YadavBelum ada peringkat
- First Trimester Bleeding and AbortionDokumen52 halamanFirst Trimester Bleeding and Abortionzahalina90Belum ada peringkat
- Universal Cranial Ultrasound Screening in Preterm Infants With Gestational Age 33 36 WeeksDokumen5 halamanUniversal Cranial Ultrasound Screening in Preterm Infants With Gestational Age 33 36 WeeksAnonymous Bx3ZJRIJFBelum ada peringkat
- Practical Atlas of Ruminant and Camelid Reproductive UltrasonographyDari EverandPractical Atlas of Ruminant and Camelid Reproductive UltrasonographyLuc DesCôteauxBelum ada peringkat
- The Accuracy of Transvaginal Ultrasonography For Early Pregnancy Diagnosis in Saanen Goats: A Pilot StudyDokumen5 halamanThe Accuracy of Transvaginal Ultrasonography For Early Pregnancy Diagnosis in Saanen Goats: A Pilot StudyYans PangerunganBelum ada peringkat
- The Safe Use of Diagnostic Ultrasound in Obstetrics and GynecologyDokumen5 halamanThe Safe Use of Diagnostic Ultrasound in Obstetrics and GynecologyshadowgardenBelum ada peringkat
- Perbandingan Usg Transvaginal Dan TransabdominalDokumen6 halamanPerbandingan Usg Transvaginal Dan TransabdominalrkyaritonangBelum ada peringkat
- Undescended TestesDokumen29 halamanUndescended TestesHillary Bushnell100% (1)
- No. 223-Content of A Complete Routine Second Trimester Obstetrical Ultrasound Examination and ReportDokumen6 halamanNo. 223-Content of A Complete Routine Second Trimester Obstetrical Ultrasound Examination and ReportYolpa Figueroa PorrasBelum ada peringkat
- 1 s2.0 S1028455911001823 MainDokumen6 halaman1 s2.0 S1028455911001823 MainFatimah AssagafBelum ada peringkat
- Obstetrical UltrasoundDokumen8 halamanObstetrical UltrasoundBerlian Purnamasari SetionoBelum ada peringkat
- Case StudyDokumen48 halamanCase Studysimbarashe tangwadzanaBelum ada peringkat
- Case Study - Uterine FibroidsDokumen9 halamanCase Study - Uterine Fibroidssimbarashe tangwadzanaBelum ada peringkat
- s13223 018 0280 7Dokumen11 halamans13223 018 0280 7SUBHADIPBelum ada peringkat
- Total Nasal Symptom ScoreDokumen1 halamanTotal Nasal Symptom ScoreLidia Shafiatul Umami100% (1)
- s13223 018 0280 7Dokumen11 halamans13223 018 0280 7SUBHADIPBelum ada peringkat
- Efek Sipatah2 Di Femur TikusDokumen10 halamanEfek Sipatah2 Di Femur TikusdellaBelum ada peringkat
- BoneDokumen21 halamanBoneAtiq RehmanBelum ada peringkat
- Sex Steroid and BoneDokumen29 halamanSex Steroid and BonedellaBelum ada peringkat
- cm2011000076 PDFDokumen10 halamancm2011000076 PDFdellaBelum ada peringkat
- Cissus Quadrangularis Plant Extract Enhances The Development of Cortical Bone and Trabeculae in The Fetal FemurDokumen21 halamanCissus Quadrangularis Plant Extract Enhances The Development of Cortical Bone and Trabeculae in The Fetal FemurdellaBelum ada peringkat
- Art:10.1007/s00534 012 0563 1Dokumen8 halamanArt:10.1007/s00534 012 0563 1Annisa Safira NurdilaBelum ada peringkat
- Competency CapacityDokumen42 halamanCompetency CapacityVaniaBelum ada peringkat
- Competency CapacityDokumen42 halamanCompetency CapacityVaniaBelum ada peringkat
- Adhd Workshop PDFDokumen2 halamanAdhd Workshop PDFshengopal8769Belum ada peringkat
- 11 - Occlusal Radiography - Pocket DentistryDokumen5 halaman11 - Occlusal Radiography - Pocket DentistryDeysi AguaguiñaBelum ada peringkat
- Pocketbookofobstetricneonatalnpediatricemergencies PDFDokumen378 halamanPocketbookofobstetricneonatalnpediatricemergencies PDFDANABelum ada peringkat
- Drug Study HaldolDokumen2 halamanDrug Study HaldolGracia EvangelistaBelum ada peringkat
- FrequencyDokumen120 halamanFrequencyp100% (1)
- Case ReportDokumen19 halamanCase ReportvivitaslimBelum ada peringkat
- Ankle Foot InjuriesDokumen85 halamanAnkle Foot InjuriesDoc DelowerBelum ada peringkat
- Using Statistical Process Control Chart Techniques To Ensure Quality of Care in Pharmacy Department of A HospitalDokumen5 halamanUsing Statistical Process Control Chart Techniques To Ensure Quality of Care in Pharmacy Department of A HospitalRezha AmaliaBelum ada peringkat
- (Doc24.vn) Bai-Tap-Tieng-Anh-10-Thi-Diem-Co-Dap-AnDokumen14 halaman(Doc24.vn) Bai-Tap-Tieng-Anh-10-Thi-Diem-Co-Dap-AnTạ Quang ĐứcBelum ada peringkat
- Radiology of Rodents, Rabbits, and Ferrets - An Atlas of Normal Anatomy and PositioningDokumen303 halamanRadiology of Rodents, Rabbits, and Ferrets - An Atlas of Normal Anatomy and PositioningCinthia RodriguezBelum ada peringkat
- Baumgaertner. The Value of The Tip-Apex Distance PDFDokumen8 halamanBaumgaertner. The Value of The Tip-Apex Distance PDFIcaruscignusBelum ada peringkat
- MPT NeurologyDokumen22 halamanMPT NeurologyDevasyaBelum ada peringkat
- Factors Influencing Customer Satisfaction in Healthcare ServicesDokumen47 halamanFactors Influencing Customer Satisfaction in Healthcare ServicesRaman ChandelBelum ada peringkat
- Enbs PanelDokumen1 halamanEnbs PanelMa'am KinBelum ada peringkat
- Health Law, Policy, and Ethics (Part 1a)Dokumen13 halamanHealth Law, Policy, and Ethics (Part 1a)omegasauronBelum ada peringkat
- IIMC PPT June 16 June FinalDokumen28 halamanIIMC PPT June 16 June FinalSumeet GoelBelum ada peringkat
- NUR1213L May2013 FinalDokumen23 halamanNUR1213L May2013 FinalOzzy Viadnes MalanaBelum ada peringkat
- Guillain-Barre Syndrome Student HandoutDokumen2 halamanGuillain-Barre Syndrome Student HandoutMiss LindiweBelum ada peringkat
- Penggunanaan Compression Stocking Terhadap Pencegahan Deep Venous Thrombosis (DVT) : Literatur ReviewDokumen5 halamanPenggunanaan Compression Stocking Terhadap Pencegahan Deep Venous Thrombosis (DVT) : Literatur ReviewElgitha BandasoBelum ada peringkat
- Report On DR.B.R.K.R Govt - Ayurvedic College & Hospital, Erragadda, HyderabadDokumen22 halamanReport On DR.B.R.K.R Govt - Ayurvedic College & Hospital, Erragadda, HyderabadRavindra Singh PalBelum ada peringkat
- Estudio Vasculatura RetinalDokumen6 halamanEstudio Vasculatura RetinalRoberto Vega FloresBelum ada peringkat
- Spinal Trauma, Imaging, Diagnosis and Management PDFDokumen1 halamanSpinal Trauma, Imaging, Diagnosis and Management PDFskeithBelum ada peringkat
- Cardiac Implant Devices MarketDokumen15 halamanCardiac Implant Devices MarketITIndustryARCBelum ada peringkat
- Umuagu Nnu DataDokumen60 halamanUmuagu Nnu DataJemilehin AbiodunBelum ada peringkat
- Standarization of Herbal DrugsDokumen8 halamanStandarization of Herbal DrugsEmmeralda PancanithaBelum ada peringkat
- 3 Perubahan Fisiologis Pada LansiaDokumen5 halaman3 Perubahan Fisiologis Pada Lansiaalbert fernandoBelum ada peringkat
- Hospital Application For Price EstimateDokumen5 halamanHospital Application For Price EstimateAndri KarundengBelum ada peringkat
- Rundown Iomu 071019 - 08.10 PDFDokumen13 halamanRundown Iomu 071019 - 08.10 PDFEfi OctavianyBelum ada peringkat
- Restraint CompetencyDokumen6 halamanRestraint CompetencyFrederick RyanBelum ada peringkat
- Scapular Dyskinesis Increases The Risk of Future Shoulder Pain by 43% in Asymptomatic Athletes A Systematic Reviwer Nad Meta AnalysisDokumen11 halamanScapular Dyskinesis Increases The Risk of Future Shoulder Pain by 43% in Asymptomatic Athletes A Systematic Reviwer Nad Meta AnalysisCesar C SBelum ada peringkat