Anda mungkin juga menyukai
- Beyond DNA: The Epigenetic Revolution: From Cellular Mechanisms to Environmental Factors: How Epigenetics Shapes Our Biological Destiny and its Implications for Health, Behavior, and the Future of ResearchDari EverandBeyond DNA: The Epigenetic Revolution: From Cellular Mechanisms to Environmental Factors: How Epigenetics Shapes Our Biological Destiny and its Implications for Health, Behavior, and the Future of ResearchBelum ada peringkat
- Insights Into The Molecular Regulatory Network of Pathomechanisms in OsteochondromaDokumen8 halamanInsights Into The Molecular Regulatory Network of Pathomechanisms in OsteochondromaEga AihenaBelum ada peringkat
- The GeneticDokumen11 halamanThe Geneticayesha rathoreBelum ada peringkat
- Developmental Genetics and Pharmacogeneticsdoc4301Dokumen8 halamanDevelopmental Genetics and Pharmacogeneticsdoc4301sayednourBelum ada peringkat
- Bone and Developement BookDokumen321 halamanBone and Developement BookGiannis Iakovou100% (4)
- Butlertjaden 2013Dokumen15 halamanButlertjaden 2013Raluca MosoiaBelum ada peringkat
- Biochemistry of GeneticsDokumen289 halamanBiochemistry of Genetics46nv7gphxzBelum ada peringkat
- Condrocyte HypertrophyDokumen9 halamanCondrocyte HypertrophyLasa SiahaanBelum ada peringkat
- A Synopsis of The Article "The Cell Biology of Bone Metabolism "Dokumen2 halamanA Synopsis of The Article "The Cell Biology of Bone Metabolism "Julina AguirreBelum ada peringkat
- EpigeneticsDokumen5 halamanEpigeneticsBioBotimy100% (1)
- Mechanisms of Obesity-Induced Male Infertility PDFDokumen24 halamanMechanisms of Obesity-Induced Male Infertility PDFshishir kumarBelum ada peringkat
- Epigenetic Control of Gene ExpressionDokumen33 halamanEpigenetic Control of Gene Expressionlordniklaus100% (1)
- Huang, 2013Dokumen38 halamanHuang, 2013wanda oktariaBelum ada peringkat
- Factors Affecting Bone GrowthDokumen7 halamanFactors Affecting Bone GrowthNurafniBelum ada peringkat
- Fcell 09 664168Dokumen13 halamanFcell 09 664168Alya RahmadaniBelum ada peringkat
- Pediatric Hand: Okta Permata Putri 71 2017 074Dokumen34 halamanPediatric Hand: Okta Permata Putri 71 2017 074Okta PermataBelum ada peringkat
- Alternative Mechanisms of Signal Transduction: The Cellular and Molecular Basis of DevelopmentDokumen32 halamanAlternative Mechanisms of Signal Transduction: The Cellular and Molecular Basis of DevelopmentDon MARSHALBelum ada peringkat
- Module 3 Biochemistry of The BrainDokumen12 halamanModule 3 Biochemistry of The BrainSakshi Jauhari100% (1)
- Review Epigenetic Codes For Heterochromatin Formation and Silencing: Rounding Up The Usual SuspectsDokumen12 halamanReview Epigenetic Codes For Heterochromatin Formation and Silencing: Rounding Up The Usual SuspectsNacido para BendcirBelum ada peringkat
- Kenkre Bassett 2018 The Bone Remodelling CycleDokumen20 halamanKenkre Bassett 2018 The Bone Remodelling Cyclealealer2708Belum ada peringkat
- Differential Gene Expression and DevelopmentDokumen9 halamanDifferential Gene Expression and DevelopmentShaher Bano Mirza100% (1)
- Epigenetics and Chromatin RemodellingDokumen30 halamanEpigenetics and Chromatin RemodellingMaya BerriesBelum ada peringkat
- The Genetic Basis of Normal and Abnormal Craniofacial Development. Acta Odontol Scand, 56 321-325, 1998Dokumen6 halamanThe Genetic Basis of Normal and Abnormal Craniofacial Development. Acta Odontol Scand, 56 321-325, 1998Muhammad AsimBelum ada peringkat
- Peran Hormon Thyroid Pada CraniofacialDokumen18 halamanPeran Hormon Thyroid Pada CraniofacialAnde Mangkuluhur Azhari ThalibbanBelum ada peringkat
- Lecture 7Dokumen19 halamanLecture 7Jamaira SamaupanBelum ada peringkat
- Cell Lines and Primary Cell Cultures in The Study of Bone Cell Biology PDFDokumen24 halamanCell Lines and Primary Cell Cultures in The Study of Bone Cell Biology PDFFilipa PereiraBelum ada peringkat
- TransposonsDokumen20 halamanTransposonsprerna tripathyBelum ada peringkat
- BSE Viva v1.0 PDFDokumen173 halamanBSE Viva v1.0 PDFKavivarma Raj RajendranBelum ada peringkat
- NIH Public Access: Author ManuscriptDokumen15 halamanNIH Public Access: Author ManuscriptMarina Milanović LBelum ada peringkat
- Epigenetics and Chromatin RemodellingDokumen30 halamanEpigenetics and Chromatin RemodellingMaxine RibeiroBelum ada peringkat
- Eosinofilos Factores de Transcripcion en Su Desarrollo Como Blanco Terapeutico Frontiers Medicine 2017Dokumen6 halamanEosinofilos Factores de Transcripcion en Su Desarrollo Como Blanco Terapeutico Frontiers Medicine 2017Gustavo GomezBelum ada peringkat
- CGJ 18 29Dokumen7 halamanCGJ 18 29ZenithaMeidaBelum ada peringkat
- Thyroid Diseases and Bone HealthDokumen11 halamanThyroid Diseases and Bone Healthmiguel saba sabaBelum ada peringkat
- Epigenetics and Aging: ReviewDokumen20 halamanEpigenetics and Aging: ReviewDeepak PanwarBelum ada peringkat
- Prenatal PDFDokumen56 halamanPrenatal PDFJohn MccormickBelum ada peringkat
- Neural Development in HumansDokumen14 halamanNeural Development in Humanssandeshi1Belum ada peringkat
- nm0699 623Dokumen6 halamannm0699 623Leonardo SalesBelum ada peringkat
- Abstract and IntroDokumen5 halamanAbstract and Intromeeegggg_Belum ada peringkat
- Advances in Biology of Orthodontic Tooth Movement - A ReviewDokumen10 halamanAdvances in Biology of Orthodontic Tooth Movement - A ReviewMarwan AlareqiBelum ada peringkat
- Kfo181 Maennl GoDokumen18 halamanKfo181 Maennl Gosong lyrics-sing your ownBelum ada peringkat
- Henry M. Kronenberg. Developmental Regulation of The Growth Plate. Nature (2003)Dokumen5 halamanHenry M. Kronenberg. Developmental Regulation of The Growth Plate. Nature (2003)Fabian BarretoBelum ada peringkat
- 678mesenquima en Desarrollo CFDokumen13 halaman678mesenquima en Desarrollo CFJuan PerezBelum ada peringkat
- Role of Cytoplasm in Cell DifferentiationDokumen7 halamanRole of Cytoplasm in Cell DifferentiationJ LALBelum ada peringkat
- Molecular Embryology of The ForegutDokumen4 halamanMolecular Embryology of The Foregutproject-247758Belum ada peringkat
- Molecular Embryology of The ForegutDokumen4 halamanMolecular Embryology of The ForegutmikeBelum ada peringkat
- Molecular Embryology of The ForegutDokumen4 halamanMolecular Embryology of The ForegutmikeBelum ada peringkat
- Molecular Embryology of The ForegutDokumen4 halamanMolecular Embryology of The ForegutmikeBelum ada peringkat
- Cell DifferentiationDokumen11 halamanCell DifferentiationMahmoud HeshamBelum ada peringkat
- Homeopathic Miasms and HeredityDokumen23 halamanHomeopathic Miasms and Heredityambertje12100% (1)
- Daluiski 2001Dokumen15 halamanDaluiski 2001Marcelo CortesBelum ada peringkat
- Slide Referat OsteochondromaDokumen14 halamanSlide Referat Osteochondromadean evansBelum ada peringkat
- Epigenetics and Psychoneuroinmunology. Mechanims and ModelsDokumen15 halamanEpigenetics and Psychoneuroinmunology. Mechanims and ModelsSparkniano HeBelum ada peringkat
- Controlling Factors in Craniofacial GrowthDokumen82 halamanControlling Factors in Craniofacial GrowthPrachodh0% (1)
- Lym, Throm, GranuDokumen12 halamanLym, Throm, Granumaxwell amponsahBelum ada peringkat
- SpermatogenesisDokumen13 halamanSpermatogenesiszuha khanBelum ada peringkat
- Cytokines IN PeriodonticsDokumen72 halamanCytokines IN PeriodonticsInduBelum ada peringkat
- Seven Types of Pleiotropy: Jonathan HodgkinDokumen5 halamanSeven Types of Pleiotropy: Jonathan HodgkinAriyo 'Jhon Jhay' IbukunBelum ada peringkat
- Cell Lines and Primary Cell Cultures in The Study of Bone Cell BiologyDokumen24 halamanCell Lines and Primary Cell Cultures in The Study of Bone Cell BiologyAngelBelum ada peringkat
- Beyond DNA: From Cellular Mechanisms to Environmental Factors: How Epigenetics Shapes Our Biological Destiny and its Implications for Health, Behavior, and the Future of ResearchDari EverandBeyond DNA: From Cellular Mechanisms to Environmental Factors: How Epigenetics Shapes Our Biological Destiny and its Implications for Health, Behavior, and the Future of ResearchBelum ada peringkat
- Osteoarthritis: (Apley + Salter)Dokumen1 halamanOsteoarthritis: (Apley + Salter)Andri KarnandaBelum ada peringkat
- The Comparison Between Two Methods For The Relief of Knee Osteoarthritis Pain Radiofrequency and Intraperiarticular OzonDokumen8 halamanThe Comparison Between Two Methods For The Relief of Knee Osteoarthritis Pain Radiofrequency and Intraperiarticular OzonAndri KarnandaBelum ada peringkat
- Minimal Important Change Values For The Oxford Knee Score and The Forgotten Joint Score at 1 Year After Total Knee ReplacementDokumen8 halamanMinimal Important Change Values For The Oxford Knee Score and The Forgotten Joint Score at 1 Year After Total Knee ReplacementAndri KarnandaBelum ada peringkat
- KDIGO 2018 Hep C GLDokumen79 halamanKDIGO 2018 Hep C GLRheeza ElhaqBelum ada peringkat
- Minimal Important Change Values For The Oxford Knee Score and The Forgotten Joint Score at 1 Year After Total Knee ReplacementDokumen8 halamanMinimal Important Change Values For The Oxford Knee Score and The Forgotten Joint Score at 1 Year After Total Knee ReplacementAndri KarnandaBelum ada peringkat
- Genicular Nerve Block For Non Acute Pain: Patient Information LeafletDokumen7 halamanGenicular Nerve Block For Non Acute Pain: Patient Information LeafletAndri KarnandaBelum ada peringkat
- Orthopaedics MCQsDokumen73 halamanOrthopaedics MCQsstillbirth100% (37)
- ADokumen1 halamanAAndri KarnandaBelum ada peringkat
- Minimal Important Change Values For The Oxford Knee Score and The Forgotten Joint Score at 1 Year After Total Knee ReplacementDokumen8 halamanMinimal Important Change Values For The Oxford Knee Score and The Forgotten Joint Score at 1 Year After Total Knee ReplacementAndri KarnandaBelum ada peringkat
- Nuh Uohj PDFDokumen166 halamanNuh Uohj PDFAndri Karnanda100% (1)
- OKSDokumen2 halamanOKSAndri KarnandaBelum ada peringkat
- ADokumen1 halamanAAndri KarnandaBelum ada peringkat
- Handbook PDFDokumen294 halamanHandbook PDFAndri KarnandaBelum ada peringkat
- Jadwal Ujian PPDS Periode Januari 2019Dokumen5 halamanJadwal Ujian PPDS Periode Januari 2019Andri KarnandaBelum ada peringkat
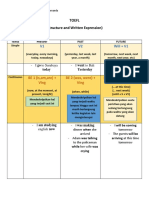
- TOEFL Written and Structure ExpressionDokumen3 halamanTOEFL Written and Structure ExpressionAndri KarnandaBelum ada peringkat
- QqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqhhhhhhhhhhhhhhhhhhhoqeeeeeeeeeeeeeeeeeeeeehttttttttttttttttttttttttttttttttkyyuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuDokumen1 halamanQqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqhhhhhhhhhhhhhhhhhhhoqeeeeeeeeeeeeeeeeeeeeehttttttttttttttttttttttttttttttttkyyuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuAndri KarnandaBelum ada peringkat
- Word Families BuildingDokumen3 halamanWord Families BuildingAndri KarnandaBelum ada peringkat
- QqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqhhhhhhhhhhhhhhhhhhhoqeeeeeeeeeeeeeeeeeeeeehttttttttttttttttttttttttttttttttkyyuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuDokumen1 halamanQqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqqhhhhhhhhhhhhhhhhhhhoqeeeeeeeeeeeeeeeeeeeeehttttttttttttttttttttttttttttttttkyyuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuAndri KarnandaBelum ada peringkat
- A Medic 40% 160 - 39 B. Bedah 20% 85 - C. Kegawat Daruratan 20% 80 - D. Kebidanan 15% 70 D. Kejiwaan 1% 4 E. Medikolegal 1Dokumen1 halamanA Medic 40% 160 - 39 B. Bedah 20% 85 - C. Kegawat Daruratan 20% 80 - D. Kebidanan 15% 70 D. Kejiwaan 1% 4 E. Medikolegal 1Andri KarnandaBelum ada peringkat
- SIMAK Pascasarjana S1 Ekstensi 2013 ENGLISH Kode 202Dokumen38 halamanSIMAK Pascasarjana S1 Ekstensi 2013 ENGLISH Kode 202Ulfi KhabibahBelum ada peringkat
- TOEFL Written and Structure ExpressionDokumen3 halamanTOEFL Written and Structure ExpressionAndri KarnandaBelum ada peringkat
- OoooooooooooooooooooooooooooooonnnnnnnnnnnnnnnnnnnnnnnnnniiiiiiiiiiiiiiiiiiiiiiiighuuuuuuuuuuuuuuuuuuuuDokumen1 halamanOoooooooooooooooooooooooooooooonnnnnnnnnnnnnnnnnnnnnnnnnniiiiiiiiiiiiiiiiiiiiiiiighuuuuuuuuuuuuuuuuuuuuAndri KarnandaBelum ada peringkat
- ggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjllllllllllllllllllllllllllllllllllllluyyyyyyyyyyyyyyyyyyyyyyyyyyyggggggggggggggllllllllllllllllll.docxDokumen1 halamanggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjjllllllllllllllllllllllllllllllllllllluyyyyyyyyyyyyyyyyyyyyyyyyyyyggggggggggggggllllllllllllllllll.docxAndri KarnandaBelum ada peringkat
- ZzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzdcsaaaaaaaaaaaaDokumen1 halamanZzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzdcsaaaaaaaaaaaaAndri KarnandaBelum ada peringkat
- CCCCCCCCCCCCCCCCCCCCCCCCCCVVVVVVVVVVVVVVVVVVVVVVVVVVVVBBBBBBBBBBBBBBBBBBBBBBBBM MmmmmmmmmmmmmmmmmmmmvvvvvvvvvvvvvvvffffffffffffffffffffffffffffyyyyyyyyyyyyyyyyyyyyyyyDokumen1 halamanCCCCCCCCCCCCCCCCCCCCCCCCCCVVVVVVVVVVVVVVVVVVVVVVVVVVVVBBBBBBBBBBBBBBBBBBBBBBBBM MmmmmmmmmmmmmmmmmmmmvvvvvvvvvvvvvvvffffffffffffffffffffffffffffyyyyyyyyyyyyyyyyyyyyyyyAndri KarnandaBelum ada peringkat
- AaaaaaaaaaaaaaaaaaaaaaaaxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxoooooooooooooooooDokumen1 halamanAaaaaaaaaaaaaaaaaaaaaaaaxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxoooooooooooooooooAndri KarnandaBelum ada peringkat
- AaaaaaaaaaaaaaaaaaaaaaaaxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxoooooooooooooooooDokumen1 halamanAaaaaaaaaaaaaaaaaaaaaaaaxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxoooooooooooooooooAndri KarnandaBelum ada peringkat
- CCCCCCCCCCCCCCCCCCCCCCCCCCVVVVVVVVVVVVVVVVVVVVVVVVVVVVBBBBBBBBBBBBBBBBBBBBBBBBM MmmmmmmmmmmmmmmmmmmmvvvvvvvvvvvvvvvffffffffffffffffffffffffffffyyyyyyyyyyyyyyyyyyyyyyyDokumen1 halamanCCCCCCCCCCCCCCCCCCCCCCCCCCVVVVVVVVVVVVVVVVVVVVVVVVVVVVBBBBBBBBBBBBBBBBBBBBBBBBM MmmmmmmmmmmmmmmmmmmmvvvvvvvvvvvvvvvffffffffffffffffffffffffffffyyyyyyyyyyyyyyyyyyyyyyyAndri KarnandaBelum ada peringkat
- CCCCCCCCCCCCCCCCCCCCCCCCCCVVVVVVVVVVVVVVVVVVVVVVVVVVVVBBBBBBBBBBBBBBBBBBBBBBBBM MmmmmmmmmmmmmmmmmmmmvvvvvvvvvvvvvvvffffffffffffffffffffffffffffyyyyyyyyyyyyyyyyyyyyyyyDokumen1 halamanCCCCCCCCCCCCCCCCCCCCCCCCCCVVVVVVVVVVVVVVVVVVVVVVVVVVVVBBBBBBBBBBBBBBBBBBBBBBBBM MmmmmmmmmmmmmmmmmmmmvvvvvvvvvvvvvvvffffffffffffffffffffffffffffyyyyyyyyyyyyyyyyyyyyyyyAndri KarnandaBelum ada peringkat
- Fbioe 08 599674Dokumen16 halamanFbioe 08 599674Tanishka AggarwalBelum ada peringkat
- TSA EpidermidisDokumen2 halamanTSA EpidermidisVi Vian HiuBelum ada peringkat
- Ar 126 eDokumen193 halamanAr 126 eKathleen ValdezBelum ada peringkat
- AP Biology Summer Packet 2020-2021Dokumen14 halamanAP Biology Summer Packet 2020-2021Ferdous Al-ShimaryBelum ada peringkat
- AllerCatPro 2.0 A Web Server For Predicting Protein Allergenicity PotentialDokumen8 halamanAllerCatPro 2.0 A Web Server For Predicting Protein Allergenicity PotentialElleBelum ada peringkat
- Angiogenesis in CancerDokumen4 halamanAngiogenesis in CanceranonymousBelum ada peringkat
- High Throughput Screening - Compound Library - Chemical Library - Screening LibraryDokumen12 halamanHigh Throughput Screening - Compound Library - Chemical Library - Screening LibrarySelleck Chemicals LLCBelum ada peringkat
- Genetic EngineeringDokumen17 halamanGenetic EngineeringBobbyBelum ada peringkat
- Lecture 2Dokumen32 halamanLecture 2alizeh amanBelum ada peringkat
- Si RNADokumen29 halamanSi RNALuis MonteroBelum ada peringkat
- Innovation in Molecular Mechanisms and Tissue EngineeringDokumen185 halamanInnovation in Molecular Mechanisms and Tissue EngineeringRenata TereniucBelum ada peringkat
- Meiosis and VariationDokumen12 halamanMeiosis and Variationsg noteBelum ada peringkat
- Feedback Loops: Glucose and Glucagon: Name: - Ishaan SinghDokumen3 halamanFeedback Loops: Glucose and Glucagon: Name: - Ishaan SinghIshaan SinghBelum ada peringkat
- Six Types of PhytoremediationDokumen5 halamanSix Types of PhytoremediationChan KianBelum ada peringkat
- Final Project 3Dokumen130 halamanFinal Project 3subhodip_k100% (1)
- Poster Urine Sediment - GBDokumen1 halamanPoster Urine Sediment - GBROBERTO CESPEDES0% (1)
- MonthlyDokumen2 halamanMonthly'Bernan Esguerra BumatayBelum ada peringkat
- Cell-Diversity LauronDokumen4 halamanCell-Diversity LauronJASMINE LAURONBelum ada peringkat
- Grade 10 Biology Week 9 Lesson 1 Worksheet 1 and Solutions PDFDokumen4 halamanGrade 10 Biology Week 9 Lesson 1 Worksheet 1 and Solutions PDFAva HoBelum ada peringkat
- MCQs For Essentials of Oral Histology and Embryology (2015) PDFDokumen199 halamanMCQs For Essentials of Oral Histology and Embryology (2015) PDFLokesh Bakshi100% (1)
- Maranatha Christian Academy SECOND Quarter Examination Science 6 I. MULTIPLE CHOICE: Choose The Letter of The Correct AnswerDokumen3 halamanMaranatha Christian Academy SECOND Quarter Examination Science 6 I. MULTIPLE CHOICE: Choose The Letter of The Correct AnswerAna GamboaBelum ada peringkat
- Topic 1 MC 1Dokumen68 halamanTopic 1 MC 1senpaiBelum ada peringkat
- Markscheme HL Paper3Dokumen8 halamanMarkscheme HL Paper3Jane ChangBelum ada peringkat
- Excretion and Homeostasis: VacuoleDokumen24 halamanExcretion and Homeostasis: Vacuolemark lwanga100% (2)
- NCERT Chapter 6: Tissues (Plant Tissue and Animal Tissue)Dokumen4 halamanNCERT Chapter 6: Tissues (Plant Tissue and Animal Tissue)Chetan Gautam100% (1)
- Bio - Chemistry T& D PaperDokumen12 halamanBio - Chemistry T& D PaperPBelum ada peringkat
- MalariaDokumen15 halamanMalariaEssa KhanBelum ada peringkat
- The Blue People of Troublesome CreekDokumen10 halamanThe Blue People of Troublesome Creekdani77660% (1)
- Genotype: Laci Laci Laci Laci Lacp Laci Laci Laco Laci Laci LacpDokumen1 halamanGenotype: Laci Laci Laci Laci Lacp Laci Laci Laco Laci Laci LacpGia HoàngBelum ada peringkat
- AN Effects of Low A260A230 012018 Ratios LRDokumen6 halamanAN Effects of Low A260A230 012018 Ratios LRAndreas HaryonoBelum ada peringkat