Anda mungkin juga menyukai
- Konsep Dasar HipotensiDokumen6 halamanKonsep Dasar HipotensididindipujaBelum ada peringkat
- Anemia Defisiensi Besi Pada Ibu HamilDokumen12 halamanAnemia Defisiensi Besi Pada Ibu HamilclaireBelum ada peringkat
- Kehamilan MolaDokumen3 halamanKehamilan MolaFitriaBelum ada peringkat
- Definisi UrolithiasisDokumen31 halamanDefinisi UrolithiasisAgung SridanaBelum ada peringkat
- DEFINISI MIOPIADokumen14 halamanDEFINISI MIOPIAAldilla Nur SukmaBelum ada peringkat
- Presentasi Kelainan RefraksiDokumen23 halamanPresentasi Kelainan RefraksiamarsyahmiBelum ada peringkat
- Cracked NippleDokumen7 halamanCracked Nipplefieolive100% (2)
- Solusio PlasentaDokumen5 halamanSolusio PlasentaEka Mailani Maya SariBelum ada peringkat
- PanggulDokumen5 halamanPanggulSofia PranaciptaBelum ada peringkat
- KONTRASEPSIDokumen68 halamanKONTRASEPSISarah Nadiya SarahBelum ada peringkat
- Kehamilan Ektopik Terganggu (Ket)Dokumen12 halamanKehamilan Ektopik Terganggu (Ket)Fachryh KonduwesBelum ada peringkat
- SK.VII.FAMED.2Dokumen34 halamanSK.VII.FAMED.2Glancius HarefaBelum ada peringkat
- Metode Amenore Laktasi (MAL) sebagai KontrasepsiDokumen18 halamanMetode Amenore Laktasi (MAL) sebagai KontrasepsieuiskurBelum ada peringkat
- Studi Kasus OligoDokumen28 halamanStudi Kasus OligoNeng Neni NurhasanahBelum ada peringkat
- Upaya Preventif Dan PromotifDokumen4 halamanUpaya Preventif Dan PromotifSuci RamadaniBelum ada peringkat
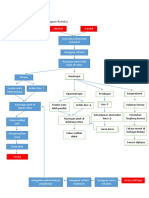
- Penanganan Perdarahan Post PartumDokumen17 halamanPenanganan Perdarahan Post PartumgloriaevasariBelum ada peringkat
- Pengertian Dan Macam-Macam Abortus KegugDokumen32 halamanPengertian Dan Macam-Macam Abortus KegugJessicaJaoBelum ada peringkat
- Modul 4 Blok 2.6Dokumen67 halamanModul 4 Blok 2.6Perdana RichyBelum ada peringkat
- Anggiks AppendicitisDokumen32 halamanAnggiks AppendicitisAndi Dhini AlfiandariBelum ada peringkat
- Pertumbuhan Janin TerhambatDokumen29 halamanPertumbuhan Janin TerhambatKrisna Yudi100% (1)
- Referat Iud ObgynDokumen22 halamanReferat Iud ObgynatikahBelum ada peringkat
- LBM 4 Mata - MeikaDokumen26 halamanLBM 4 Mata - Meikadia_iiBelum ada peringkat
- Tata Laksana Blighted OvumDokumen4 halamanTata Laksana Blighted OvumSitiBelum ada peringkat
- Nutrisi Ibu HamilDokumen15 halamanNutrisi Ibu HamilTaufiq MantoBelum ada peringkat
- Skenario 1 Modul 2 PBL OnkologiDokumen24 halamanSkenario 1 Modul 2 PBL OnkologiNahla Zaimah jainuddinBelum ada peringkat
- Patofisiologi Gangguan RefraksiDokumen3 halamanPatofisiologi Gangguan RefraksiFrifiyant AnandaBelum ada peringkat
- 1.anatomi Dan Fisiologi Payudara.Dokumen15 halaman1.anatomi Dan Fisiologi Payudara.AINIBelum ada peringkat
- Anatomi dan Fisiologi PlasentaDokumen11 halamanAnatomi dan Fisiologi PlasentaDesima Tamara sinuratBelum ada peringkat
- BBDM Kelompok 14 Modul 6 - Skenario 1Dokumen29 halamanBBDM Kelompok 14 Modul 6 - Skenario 1Evelyn MeilianiBelum ada peringkat
- Askep Bercak MongolDokumen9 halamanAskep Bercak MongolmutiBelum ada peringkat
- DIAGNOSADokumen39 halamanDIAGNOSAsanti dwi cBelum ada peringkat
- Makalah - Fisiologi MenstruasiDokumen9 halamanMakalah - Fisiologi Menstruasianfadillah77Belum ada peringkat
- Pathofisiologi Dan Rehabilitasi Medik Pada Osteoporosis2Dokumen12 halamanPathofisiologi Dan Rehabilitasi Medik Pada Osteoporosis2Nuriana Al-BanjaryBelum ada peringkat
- Lapkas OBSGYN HRPDokumen51 halamanLapkas OBSGYN HRPettorebugattiBelum ada peringkat
- Rupture Uteri - Fatima KNDokumen22 halamanRupture Uteri - Fatima KNnisakhiarunBelum ada peringkat
- Inervasi OrbitaDokumen32 halamanInervasi Orbitanurhana100% (1)
- Anatomi AdnexaDokumen4 halamanAnatomi Adnexaidhaa_siregarBelum ada peringkat
- Presentasi Bokong ReviisipptDokumen51 halamanPresentasi Bokong ReviisipptOna Putra KarisnaBelum ada peringkat
- Phantom Manual PlasentaDokumen24 halamanPhantom Manual PlasentaSylvia PertiwiBelum ada peringkat
- SalpingitisDokumen9 halamanSalpingitisLuchy AnBelum ada peringkat
- Referat PcosDokumen19 halamanReferat PcosAnonymous 0IhyCagff4Belum ada peringkat
- Persalinan AbnormalDokumen5 halamanPersalinan AbnormalElfha MonitaBelum ada peringkat
- REPRODUKSI PRIADokumen17 halamanREPRODUKSI PRIATheva LoloBelum ada peringkat
- Laporan PBL Bab Encer TerbaruDokumen53 halamanLaporan PBL Bab Encer TerbaruAndi Dian HajrianaBelum ada peringkat
- Pubertas TardaDokumen15 halamanPubertas TardaJoshuaRobertoPratamaBelum ada peringkat
- MENGATASI INFERTILITASDokumen21 halamanMENGATASI INFERTILITASBomi YoonBelum ada peringkat
- INFERTILITAS SEKUNDERDokumen28 halamanINFERTILITAS SEKUNDERSuciPurnamarzaBelum ada peringkat
- 3 Landasan Teori DismenoreaDokumen6 halaman3 Landasan Teori DismenoreaRNofian Nak UnSuBelum ada peringkat
- LAPORAN KASUS POSTDATEDokumen53 halamanLAPORAN KASUS POSTDATEdark cloverBelum ada peringkat
- Case Report KPDDokumen21 halamanCase Report KPDTito Haposan TobingBelum ada peringkat
- Missed AbortionDokumen15 halamanMissed AbortionIfa MarlinaBelum ada peringkat
- Lo 5 Diagnosis Dan Diagnosis Banding Infeksi Saluran KemihDokumen8 halamanLo 5 Diagnosis Dan Diagnosis Banding Infeksi Saluran KemihErica DinataBelum ada peringkat
- SK 1 - Kesehatan Ibu Anak Dan RemajaDokumen14 halamanSK 1 - Kesehatan Ibu Anak Dan RemajaNovi SeptianiBelum ada peringkat
- IkterusDokumen7 halamanIkterusAnggita PrawyandaniBelum ada peringkat
- PUA-Definisi,Epidemiologi,Etiologi,Diagnosa,PengobatanDokumen10 halamanPUA-Definisi,Epidemiologi,Etiologi,Diagnosa,PengobatanKhairunnisa SodikinBelum ada peringkat
- TUMOR JINAK REPRODUKSIDokumen21 halamanTUMOR JINAK REPRODUKSIRUDI MOTORBelum ada peringkat
- MIOPIADokumen4 halamanMIOPIAThina KrishnanBelum ada peringkat
- Keratitis KorneaDokumen29 halamanKeratitis KornearahmanBelum ada peringkat
- Hiperemesis GravidarumDokumen54 halamanHiperemesis Gravidarumujianterpusat 2022Belum ada peringkat
- Nausea FixDokumen4 halamanNausea FixPutri AzkiaBelum ada peringkat
- Analsis Swot Dan IntervensinyaDokumen3 halamanAnalsis Swot Dan IntervensinyaAgatha Qyara AnnabellaBelum ada peringkat
- Dokter Keluarga Dan Bpjs KesehatanDokumen24 halamanDokter Keluarga Dan Bpjs KesehatanAgatha Qyara AnnabellaBelum ada peringkat
- Permenkes No 75 TH 2014 TTG PuskesmasDokumen24 halamanPermenkes No 75 TH 2014 TTG PuskesmasAnonymous bwyPj8QB67% (3)
- Gangguan Waham MenetapDokumen12 halamanGangguan Waham MenetapAgatha Qyara AnnabellaBelum ada peringkat
- Bab I PendahuluanDokumen8 halamanBab I PendahuluanAgatha Qyara AnnabellaBelum ada peringkat
- Aspek Medikolegal Pelayanan Gawat DaruratDokumen4 halamanAspek Medikolegal Pelayanan Gawat DaruratropusanBelum ada peringkat
- Diagnosis Gangguan JiwaDokumen172 halamanDiagnosis Gangguan Jiwasohbah90% (52)
- Asam Nukleat Dan SintesisDokumen55 halamanAsam Nukleat Dan SintesisAgatha Qyara AnnabellaBelum ada peringkat
- Hubungan Lama Kemoterapi Dengan Konsep Diri Pasien Kanker PayudaraDokumen15 halamanHubungan Lama Kemoterapi Dengan Konsep Diri Pasien Kanker PayudaraAgatha Qyara AnnabellaBelum ada peringkat
- Asam Nukleat Dan SintesisDokumen55 halamanAsam Nukleat Dan SintesisAgatha Qyara AnnabellaBelum ada peringkat
- Kisi-Kisi Uas KimiaDokumen8 halamanKisi-Kisi Uas KimiaAgatha Qyara AnnabellaBelum ada peringkat
- Angket KtiDokumen2 halamanAngket KtiAgatha Qyara AnnabellaBelum ada peringkat
- Laporan Biologi NutrisiDokumen10 halamanLaporan Biologi NutrisiAgatha Qyara AnnabellaBelum ada peringkat
- Pemanasan Global (Isi)Dokumen4 halamanPemanasan Global (Isi)Agatha Qyara AnnabellaBelum ada peringkat
- Kinetik GasDokumen20 halamanKinetik GasAgatha Qyara AnnabellaBelum ada peringkat
- Enzim DasarDokumen10 halamanEnzim Dasarngulmi.khamidahBelum ada peringkat
- Pemanasan Global (Cover)Dokumen1 halamanPemanasan Global (Cover)Agatha Qyara AnnabellaBelum ada peringkat
- Ekonomi BumdDokumen9 halamanEkonomi BumdAgatha Qyara AnnabellaBelum ada peringkat
- 7 Jump NewDokumen7 halaman7 Jump NewAgatha Qyara AnnabellaBelum ada peringkat
- Kelapangan Hati dan Kemudahan Setelah KesulitanDokumen10 halamanKelapangan Hati dan Kemudahan Setelah KesulitanAgatha Qyara AnnabellaBelum ada peringkat
- Soal Biologi SmaDokumen11 halamanSoal Biologi SmaAgatha Qyara AnnabellaBelum ada peringkat
- Q.S. Al-Insyirah 1-8Dokumen11 halamanQ.S. Al-Insyirah 1-8Agatha Qyara AnnabellaBelum ada peringkat
- Teks EditorialDokumen10 halamanTeks EditorialAgatha Qyara AnnabellaBelum ada peringkat
- 7 Jump NewDokumen7 halaman7 Jump NewAgatha Qyara AnnabellaBelum ada peringkat
- FirstDokumen6 halamanFirstAgatha Qyara AnnabellaBelum ada peringkat
- Bab 2 Tinjauan Pustaka 2.1. Air Susu Ibu (ASI) Eksklusif: SeizuresDokumen12 halamanBab 2 Tinjauan Pustaka 2.1. Air Susu Ibu (ASI) Eksklusif: SeizuresAgatha Qyara AnnabellaBelum ada peringkat
- 1st DayDokumen1 halaman1st DayAgatha Qyara AnnabellaBelum ada peringkat
- The TheoryDokumen12 halamanThe TheoryAgatha Qyara AnnabellaBelum ada peringkat
- SINDROM KLINEFELTER Tutorial BlokDokumen12 halamanSINDROM KLINEFELTER Tutorial BlokAgatha Qyara AnnabellaBelum ada peringkat