Anda mungkin juga menyukai
- Thinking Skills and Problem Solving Oum Jan 2020Dokumen15 halamanThinking Skills and Problem Solving Oum Jan 2020Shoba ManoharanBelum ada peringkat
- Intestine ObstructionDokumen37 halamanIntestine ObstructionGoesti YudistiraBelum ada peringkat
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeDari EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeBelum ada peringkat
- No Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [III EDITION]Dari EverandNo Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [III EDITION]Penilaian: 5 dari 5 bintang5/5 (24)
- Fluid Therapy in Dengue CPG Modify HPP 2017Dokumen37 halamanFluid Therapy in Dengue CPG Modify HPP 2017Nur FadzilahBelum ada peringkat
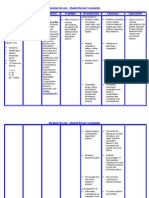
- NURSING CARE PLAN - Liver CirrhosisDokumen2 halamanNURSING CARE PLAN - Liver Cirrhosisderic100% (27)
- Nclex Pharm TipsDokumen39 halamanNclex Pharm TipsPohs Enilno100% (18)
- Bowel Obstruction: Timothy M. Farrell Department of Surgery UNC-Chapel HillDokumen27 halamanBowel Obstruction: Timothy M. Farrell Department of Surgery UNC-Chapel HillBheru LalBelum ada peringkat
- Dr. H. Achmad Fuadi, SPB-KBD, MkesDokumen47 halamanDr. H. Achmad Fuadi, SPB-KBD, MkesytreiiaaBelum ada peringkat
- Patients With Noninflammatory Intestinal Disorders: UPNS 232 Adult Health and IllnessDokumen41 halamanPatients With Noninflammatory Intestinal Disorders: UPNS 232 Adult Health and Illnesslucas dibenedettoBelum ada peringkat
- Intestinal ObstructionDokumen19 halamanIntestinal ObstructionAna-Maria OchialbiBelum ada peringkat
- Instestinal Obstruction UbthDokumen34 halamanInstestinal Obstruction UbthDonald IDEDEBelum ada peringkat
- Bowel ObstructionDokumen36 halamanBowel ObstructionyoanBelum ada peringkat
- 1100 Ultrasound of The Acute Abdomen 15 3Dokumen84 halaman1100 Ultrasound of The Acute Abdomen 15 3gp1promo2016Belum ada peringkat
- Gastric Outlet ObstructionDokumen59 halamanGastric Outlet Obstructionmaryam tariqBelum ada peringkat
- Intestinal Obstruction CME CYYDokumen36 halamanIntestinal Obstruction CME CYYSofiuddin Bin NordinBelum ada peringkat
- Large Bowel ObstructionDokumen36 halamanLarge Bowel Obstructionpuleng matshabaBelum ada peringkat
- GIS-K-26 Intestinal Obstruction: Syahbudin HarahapDokumen23 halamanGIS-K-26 Intestinal Obstruction: Syahbudin Harahaplidz_margaretBelum ada peringkat
- Ileus ObstructionDokumen22 halamanIleus ObstructionfitrahBelum ada peringkat
- Presentation CMCDokumen49 halamanPresentation CMCrima othmanBelum ada peringkat
- Neonatal Intestinal Obstruction EPSGHAN PDFDokumen77 halamanNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenBelum ada peringkat
- Acute Intestinal Obstruction...Dokumen42 halamanAcute Intestinal Obstruction...Ali100% (2)
- Colon 2Dokumen56 halamanColon 2EnydLaRejBelum ada peringkat
- Bowel ObstructionDokumen48 halamanBowel ObstructionPatrick John100% (1)
- Large Bowel Obstruction by Nic MDokumen42 halamanLarge Bowel Obstruction by Nic MRisky OpponentBelum ada peringkat
- Abdominal Pain, Vomitting & ConstipationDokumen77 halamanAbdominal Pain, Vomitting & ConstipationShermin ShakilBelum ada peringkat
- Nursing Stomach NotesDokumen5 halamanNursing Stomach Noteslucas dibenedettoBelum ada peringkat
- Abnormalities in Small Bowel: Dr. Iqbal Pahlevi, SPB, SpbaDokumen36 halamanAbnormalities in Small Bowel: Dr. Iqbal Pahlevi, SPB, SpbafinikollinsBelum ada peringkat
- Intestinal ObstructionDokumen47 halamanIntestinal ObstructionAstrid Kurniawati AyuningtyasBelum ada peringkat
- Intestinal Obstruction...Dokumen26 halamanIntestinal Obstruction...Yonathan asnakeBelum ada peringkat
- VolvulusDokumen38 halamanVolvulusHector RaulBelum ada peringkat
- Abdominal Emergencies Presentation (Recovered)Dokumen126 halamanAbdominal Emergencies Presentation (Recovered)kityamuwesiBelum ada peringkat
- Approach To Abdominal Pain in EDDokumen29 halamanApproach To Abdominal Pain in EDAneeq Nayer KhanBelum ada peringkat
- CME - Dr. Amarchand Bajaj (Revised)Dokumen19 halamanCME - Dr. Amarchand Bajaj (Revised)Rahul AryaBelum ada peringkat
- Abdominal Emergencies 1Dokumen29 halamanAbdominal Emergencies 1kecemasan taipingBelum ada peringkat
- Abdominal Wall Defects: Dr. Catherine B. CaneteDokumen42 halamanAbdominal Wall Defects: Dr. Catherine B. CaneteLuqman AlwiBelum ada peringkat
- Atresia BilierDokumen41 halamanAtresia Bilierrizka hastari100% (1)
- Obstruksi IntestinalDokumen37 halamanObstruksi IntestinalkrisandiBelum ada peringkat
- Intestinalobstruction 150401053831 Conversion Gate01Dokumen65 halamanIntestinalobstruction 150401053831 Conversion Gate01Nina NoviaBelum ada peringkat
- Recent Management of Calculous Biliary DiseaseDokumen35 halamanRecent Management of Calculous Biliary DiseaseAbhishek SarafBelum ada peringkat
- Blunt Abdomen Trauma FixDokumen22 halamanBlunt Abdomen Trauma FixUlfa Rahmadanti SetiawanBelum ada peringkat
- 7.intestinal ObstruDokumen42 halaman7.intestinal Obstrujitendra magarBelum ada peringkat
- Congenital Bowel ObstructionsDokumen33 halamanCongenital Bowel ObstructionsMpanso Ahmad AlhijjBelum ada peringkat
- Large Bowel Obstruction: Katherine Jahnes MD Colorectal Conference ST Luke's Roosevelt Hospital Center November 10, 2005Dokumen22 halamanLarge Bowel Obstruction: Katherine Jahnes MD Colorectal Conference ST Luke's Roosevelt Hospital Center November 10, 2005samsabesBelum ada peringkat
- Kelainan Pada Usus HalusDokumen28 halamanKelainan Pada Usus HalusClara Shinta AruanBelum ada peringkat
- Intestinal ObstructionDokumen52 halamanIntestinal ObstructionAsfandyar Khan100% (2)
- Pediatrics Surgery I: Presenter: Osoro Yvonne Kwamboka Facilitator: DR Wairimu NdegwaDokumen24 halamanPediatrics Surgery I: Presenter: Osoro Yvonne Kwamboka Facilitator: DR Wairimu NdegwaMalueth AnguiBelum ada peringkat
- Acute Intestinal ObstructionDokumen50 halamanAcute Intestinal ObstructionDin LukbanBelum ada peringkat
- Bowel Obstruction - ppt1Dokumen30 halamanBowel Obstruction - ppt1Elfrida Aulia100% (1)
- Intestinal Obstruction2Dokumen26 halamanIntestinal Obstruction2TwinkleBelum ada peringkat
- Abdominal Pain: Kerut SuardanaDokumen48 halamanAbdominal Pain: Kerut SuardanaDiah SandiBelum ada peringkat
- Acute Abdomen: Part I: Intestinal Obstruction/Bowel Infarction/ Constipation (And How To Assess and Initiate Management)Dokumen63 halamanAcute Abdomen: Part I: Intestinal Obstruction/Bowel Infarction/ Constipation (And How To Assess and Initiate Management)Rumana IslamBelum ada peringkat
- Biliary Tract DiseaseDokumen52 halamanBiliary Tract DiseaseAna Cotoman100% (1)
- Biliary Atresia: Dr. Boris Crossley NainggolanDokumen41 halamanBiliary Atresia: Dr. Boris Crossley Nainggolanrizka hastariBelum ada peringkat
- 8 28 12 R Schaffer MDDokumen51 halaman8 28 12 R Schaffer MDKay BristolBelum ada peringkat
- Intestinal ObstructionDokumen48 halamanIntestinal ObstructionMahmoud AbuAwadBelum ada peringkat
- Abdominal Pain: James S Newman, M.D. The University of Texas Medical BranchDokumen27 halamanAbdominal Pain: James S Newman, M.D. The University of Texas Medical BranchYudiese YouBelum ada peringkat
- Intestinal Obstruction: by Dr. Shereen Abd El-MoniemDokumen44 halamanIntestinal Obstruction: by Dr. Shereen Abd El-MoniemフセインBelum ada peringkat
- General Surgery SMALL INTESTINES-Dr MendozaDokumen101 halamanGeneral Surgery SMALL INTESTINES-Dr MendozaMedisina101Belum ada peringkat
- Abdominal Pain: LSU Medical Student Clerkship, New Orleans, LADokumen48 halamanAbdominal Pain: LSU Medical Student Clerkship, New Orleans, LALeonardo Adi BestBelum ada peringkat
- Gall StonesDokumen26 halamanGall StonesNia SinghBelum ada peringkat
- Neonatal Intestinal Obstruction (Nuha Khwaja)Dokumen21 halamanNeonatal Intestinal Obstruction (Nuha Khwaja)dtalks andyouBelum ada peringkat
- Thrombocytopaenia in Pregnancy: DR Guan Yong Khee Hospital MelakaDokumen40 halamanThrombocytopaenia in Pregnancy: DR Guan Yong Khee Hospital MelakaNur Fadzilah100% (1)
- CPGS: Management of Immune Thrombocytopaenic Purpura: DR Zanapiah Zakaria Haematology Update 2007 Hospital AmpangDokumen33 halamanCPGS: Management of Immune Thrombocytopaenic Purpura: DR Zanapiah Zakaria Haematology Update 2007 Hospital AmpangNur FadzilahBelum ada peringkat
- Intestinal Obstruction (PBL) (Teaching)Dokumen40 halamanIntestinal Obstruction (PBL) (Teaching)Nur FadzilahBelum ada peringkat
- Approach To The Patient With Shortness of Breath: Colin EdwardsDokumen37 halamanApproach To The Patient With Shortness of Breath: Colin EdwardsNur FadzilahBelum ada peringkat
- Frozen ShoulderDokumen9 halamanFrozen ShoulderNur FadzilahBelum ada peringkat
- Uts 1 Farmakologi - Blok Neuroscience Kamis, 14 Oktober 2010Dokumen4 halamanUts 1 Farmakologi - Blok Neuroscience Kamis, 14 Oktober 2010Nur FadzilahBelum ada peringkat
- Clinical Appearance of Oral Lesions in Bronchial Asthma Patients Using Inhalation DrugDokumen7 halamanClinical Appearance of Oral Lesions in Bronchial Asthma Patients Using Inhalation DrugDenna Idryareza AugustyanaBelum ada peringkat
- Jurnal Terapi Komprehensif HipertensiDokumen4 halamanJurnal Terapi Komprehensif HipertensiismiBelum ada peringkat
- Cynovial Fluid: by Dr. Gouse Mohiddin ShaikDokumen20 halamanCynovial Fluid: by Dr. Gouse Mohiddin ShaikLaverne MarceloBelum ada peringkat
- Charcot-Marie-Tooth DiseaseDokumen2 halamanCharcot-Marie-Tooth DiseaseitsmeayaeBelum ada peringkat
- NCM Digestive 2 PDFDokumen11 halamanNCM Digestive 2 PDFsamantha lumapasBelum ada peringkat
- WCPD 2016 CP Diagnosis Treatment Infographic WORLDDokumen1 halamanWCPD 2016 CP Diagnosis Treatment Infographic WORLDvinicius_vrrBelum ada peringkat
- NCP For Ineffective Airway ClearanceDokumen3 halamanNCP For Ineffective Airway ClearanceJennelyn BayleBelum ada peringkat
- VT TestingDokumen5 halamanVT Testinggogo36Belum ada peringkat
- Letter To ACS CommissionerDokumen4 halamanLetter To ACS CommissionerCity Limits (New York)Belum ada peringkat
- World Diabetes DayDokumen48 halamanWorld Diabetes DaykavithagopalBelum ada peringkat
- Diabetes Flow ChartDokumen8 halamanDiabetes Flow ChartNicky ChhajwaniBelum ada peringkat
- Benefits of ExerciseDokumen11 halamanBenefits of ExerciseNur JuwainaBelum ada peringkat
- 21-Article Text-28-1-10-20180319Dokumen11 halaman21-Article Text-28-1-10-20180319Diantika PutriBelum ada peringkat
- Age NCPDokumen3 halamanAge NCPMartin Allen ClaudioBelum ada peringkat
- Kuliah 16 Cor PulmonaleDokumen41 halamanKuliah 16 Cor PulmonalecaturwiraBelum ada peringkat
- Undo It!: How Simple Lifestyle Changes Can Reverse Most Chronic Diseases - Dean Ornish M.D.Dokumen5 halamanUndo It!: How Simple Lifestyle Changes Can Reverse Most Chronic Diseases - Dean Ornish M.D.besahahu7% (15)
- Cardio Nancy Test BankDokumen36 halamanCardio Nancy Test BankNoavilBelum ada peringkat
- Health Teaching PlanDokumen12 halamanHealth Teaching PlanFrancis SorianoBelum ada peringkat
- History of Psychiatry 2007 Engstrom 389 98Dokumen11 halamanHistory of Psychiatry 2007 Engstrom 389 98fgtwhblwednwlkBelum ada peringkat
- Crohn's DiseaseDokumen46 halamanCrohn's Diseaseuttarasingh100% (3)
- CWU OrthopedicsDokumen6 halamanCWU OrthopedicsSana Anam JahanBelum ada peringkat
- Artificial AirwaysDokumen17 halamanArtificial AirwaysSri DarmayantiBelum ada peringkat
- Allan Ocampo Tutorials: Mobile:0920-5583476 Bus.:273-2245Dokumen55 halamanAllan Ocampo Tutorials: Mobile:0920-5583476 Bus.:273-2245ocampotutorials100% (1)
- Chapter " I" Multiple Choice QuestionsDokumen56 halamanChapter " I" Multiple Choice QuestionsFiras AnayaBelum ada peringkat
- MeningoencephaloceleDokumen13 halamanMeningoencephaloceleIda Bagus Yudha Prasista100% (1)
- Running Head: Article Critique 1Dokumen5 halamanRunning Head: Article Critique 1Clifford OmondiBelum ada peringkat
- Drug Study - LosartanDokumen2 halamanDrug Study - LosartanCath Bril50% (2)



![No Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [III EDITION]](https://imgv2-2-f.scribdassets.com/img/word_document/591540228/149x198/6ba6cc3b38/1713999276?v=1)