Anda mungkin juga menyukai
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtDari EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtPenilaian: 5 dari 5 bintang5/5 (1)
- CHFDokumen35 halamanCHFireneBelum ada peringkat
- CHFDokumen45 halamanCHFAry 01Belum ada peringkat
- CHFDokumen22 halamanCHFshazia kaziBelum ada peringkat
- Congestive Heart FailureDokumen25 halamanCongestive Heart FailuredevianiamalinaBelum ada peringkat
- Heart FailureDokumen22 halamanHeart FailureYoussef MansourBelum ada peringkat
- Heart Failure: DR Kaem Shir AliDokumen24 halamanHeart Failure: DR Kaem Shir AliMwanja MosesBelum ada peringkat
- Heart Failure GuideDokumen8 halamanHeart Failure GuideAikoP.NarcisoBelum ada peringkat
- Congestive Heart FailureDokumen28 halamanCongestive Heart Failuresarguss1480% (5)
- Cardiac Failure: Dr. Abdul Ghani WaseemDokumen33 halamanCardiac Failure: Dr. Abdul Ghani WaseemFarwaBelum ada peringkat
- Congestive Heart Failure ReportDokumen6 halamanCongestive Heart Failure ReportSunshine_Bacla_4275100% (1)
- Essential Guide to Heart FailureDokumen59 halamanEssential Guide to Heart FailureMahesh RathnayakeBelum ada peringkat
- Cardiac Failure Diagnosis and TreatmentDokumen5 halamanCardiac Failure Diagnosis and TreatmentMatyie SmkasBelum ada peringkat
- Heart Failure: Understanding the Definition, Causes, Symptoms and TreatmentDokumen48 halamanHeart Failure: Understanding the Definition, Causes, Symptoms and TreatmentSanjay SathasevanBelum ada peringkat
- Congestive Cardiac FailureDokumen38 halamanCongestive Cardiac FailureSalman KhanBelum ada peringkat
- HeartFailure Nursing FIK 2014Dokumen101 halamanHeartFailure Nursing FIK 2014Putri NurlaeliBelum ada peringkat
- Chinonye Ekeocha, Tazleem Khan, Ogechi Ekeocha August 23, 2010 Jackson Park Hospital Internal Medicine Core ClerkshipDokumen31 halamanChinonye Ekeocha, Tazleem Khan, Ogechi Ekeocha August 23, 2010 Jackson Park Hospital Internal Medicine Core ClerkshipsgolbariBelum ada peringkat
- Heart FailureDokumen17 halamanHeart FailureIsna IndahBelum ada peringkat
- DR Harris Hasan SPPD, SPJP (K) Departemen Kardiologi FK Usu MedanDokumen46 halamanDR Harris Hasan SPPD, SPJP (K) Departemen Kardiologi FK Usu MedanAndi WiraBelum ada peringkat
- Gagal JantungDokumen54 halamanGagal JantungMiftahul IfahBelum ada peringkat
- 4 - (CHF), IschemicDokumen31 halaman4 - (CHF), IschemicLobna ElkilanyBelum ada peringkat
- Cardiac Heart Failure Guide: Causes, Symptoms & Nursing CareDokumen43 halamanCardiac Heart Failure Guide: Causes, Symptoms & Nursing CareCindy DeliaBelum ada peringkat
- Congestive Heart Failure pptDokumen21 halamanCongestive Heart Failure pptsubhashreepal700Belum ada peringkat
- DR Harris Hasan SPPD, SPJP (K) Departemen Kardiologi FK Usu MedanDokumen46 halamanDR Harris Hasan SPPD, SPJP (K) Departemen Kardiologi FK Usu MedanAziz DjohariBelum ada peringkat
- Heart FailureDokumen39 halamanHeart FailureMuhammad AsifBelum ada peringkat
- Congestive Heart FailureDokumen12 halamanCongestive Heart Failuresubhashreepal700Belum ada peringkat
- Heart To HeartDokumen110 halamanHeart To HeartmahyorwaBelum ada peringkat
- HEART FAILURE: CAUSES, DIAGNOSIS AND TREATMENTDokumen48 halamanHEART FAILURE: CAUSES, DIAGNOSIS AND TREATMENTAlbert SitepuBelum ada peringkat
- Congestive Cardiac FailureDokumen20 halamanCongestive Cardiac FailureAnand VaghasiyaBelum ada peringkat
- Thursday Nov 3rd - BayehDokumen12 halamanThursday Nov 3rd - BayehFatima MaazBelum ada peringkat
- Heart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDokumen42 halamanHeart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik Medanbilli lisanuddinBelum ada peringkat
- Heart Failure: Kalaiselvan OtDokumen46 halamanHeart Failure: Kalaiselvan Otplayme_nowBelum ada peringkat
- Ipd - KardiologiDokumen116 halamanIpd - KardiologiWynda MuljonoBelum ada peringkat
- Comprehensive Study of Beta BlockersDokumen40 halamanComprehensive Study of Beta Blockersapi-369859880% (5)
- Heart Failure: DR - Liu LixinDokumen46 halamanHeart Failure: DR - Liu LixinsanjivdasBelum ada peringkat
- Heart Failure: Causes, Symptoms, Diagnosis and TreatmentDokumen46 halamanHeart Failure: Causes, Symptoms, Diagnosis and TreatmentRamli HusenBelum ada peringkat
- Congestive Heart FailureDokumen39 halamanCongestive Heart FailureEthiopia TekdemBelum ada peringkat
- Heart Failure & Cardiac Arrest: Rony YuliwansyahDokumen92 halamanHeart Failure & Cardiac Arrest: Rony YuliwansyahSasha ManoBelum ada peringkat
- Heart Failure: Presentation by Dr. Tooba ShahbazDokumen30 halamanHeart Failure: Presentation by Dr. Tooba ShahbazTooba ShahbazBelum ada peringkat
- Types Heart Failure PDFDokumen10 halamanTypes Heart Failure PDFHannaBelum ada peringkat
- 8A - Heart FailureDokumen114 halaman8A - Heart FailureShahpoor Ahmad ShirzadaBelum ada peringkat
- CHF Blok KardiovaskularDokumen39 halamanCHF Blok KardiovaskularAnonymous Cz5xlxyU9VBelum ada peringkat
- Hypertension & Congestif Heart FailureDokumen25 halamanHypertension & Congestif Heart FailureDeriIrvantoBelum ada peringkat
- KP 2.5.5.1 Gagal Jantung KronikDokumen39 halamanKP 2.5.5.1 Gagal Jantung Kronikayam kecapBelum ada peringkat
- Heart Failure NewDokumen31 halamanHeart Failure NewMeeraBelum ada peringkat
- heart failure الاخيرDokumen30 halamanheart failure الاخيرAliBelum ada peringkat
- Congestive Heart Failure PDFDokumen11 halamanCongestive Heart Failure PDFpriyanka bhavsarBelum ada peringkat
- P 3a Gagal JTGDokumen35 halamanP 3a Gagal JTGAnaMariyaMaBelum ada peringkat
- HEART FAILURE: SYMPTOMS, CAUSES AND TREATMENTDokumen39 halamanHEART FAILURE: SYMPTOMS, CAUSES AND TREATMENTnurul ramadhiniBelum ada peringkat
- Manage Cardiac EmergenciesDokumen56 halamanManage Cardiac Emergencies21rayhanf100% (1)
- Heart FailureDokumen30 halamanHeart FailureYopih YohanesBelum ada peringkat
- Cardiomyopathy (21 4 9)Dokumen59 halamanCardiomyopathy (21 4 9)Moush AbdiBelum ada peringkat
- Congestive Heart FailureDokumen14 halamanCongestive Heart Failurelolo0880Belum ada peringkat
- Heart Failure: Mohammad DiahDokumen50 halamanHeart Failure: Mohammad DiahAdityaBelum ada peringkat
- Seminar On Heart Failure: Presented by Neethu.MDokumen59 halamanSeminar On Heart Failure: Presented by Neethu.MNeethu JayasankarBelum ada peringkat
- CARDIOMYOPATHYDokumen18 halamanCARDIOMYOPATHYChiqui YumangBelum ada peringkat
- Atrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesDari EverandAtrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesPenilaian: 4 dari 5 bintang4/5 (1)
- Cardiac Care and COVID-19: Perspectives in Medical PracticeDari EverandCardiac Care and COVID-19: Perspectives in Medical PracticeBelum ada peringkat
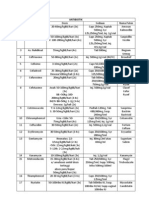
- Daftar Dosis Dan Sediaan ObatDokumen5 halamanDaftar Dosis Dan Sediaan ObatVenessa Rudy Pranata97% (38)
- 1.1. Krisis Hipertensi - Dr. Saugi AbduhDokumen29 halaman1.1. Krisis Hipertensi - Dr. Saugi AbduhdmaulidaBelum ada peringkat
- Naskah PublikasiDokumen16 halamanNaskah PublikasiAsep MkgtaBelum ada peringkat
- Naskah PublikasiDokumen16 halamanNaskah PublikasiAsep MkgtaBelum ada peringkat
- Acute Scrotum PDFDokumen16 halamanAcute Scrotum PDFRangga Alam VaneoBelum ada peringkat
- Naskah PublikasiDokumen16 halamanNaskah PublikasiAsep MkgtaBelum ada peringkat
- Paediatrica Indonesiana: Original ArticleDokumen5 halamanPaediatrica Indonesiana: Original ArticleScribdMeUpBelum ada peringkat
- Paediatrica Indonesiana: Original ArticleDokumen5 halamanPaediatrica Indonesiana: Original ArticleScribdMeUpBelum ada peringkat
- Daftar Kelulusan Mcqs CBT Ukmppd Periode Agustus 2019Dokumen113 halamanDaftar Kelulusan Mcqs CBT Ukmppd Periode Agustus 2019FarhanBelum ada peringkat
- ANAPHYLAXISDokumen14 halamanANAPHYLAXISRangga Alam VaneoBelum ada peringkat
- Daftar Dosis Dan Sediaan ObatDokumen5 halamanDaftar Dosis Dan Sediaan ObatVenessa Rudy Pranata97% (38)
- Pancreatic Tumors PDFDokumen9 halamanPancreatic Tumors PDFRangga Alam VaneoBelum ada peringkat
- 1.1. Krisis Hipertensi - Dr. Saugi AbduhDokumen29 halaman1.1. Krisis Hipertensi - Dr. Saugi AbduhdmaulidaBelum ada peringkat
- Kelulusan Ukmppd Feb 2018Dokumen124 halamanKelulusan Ukmppd Feb 2018Dexel Putra SimbolonBelum ada peringkat
- Diagnosing Acute Appendicitis PDFDokumen7 halamanDiagnosing Acute Appendicitis PDFIstigfarani InBelum ada peringkat
- Diagnosing Acute Appendicitis PDFDokumen7 halamanDiagnosing Acute Appendicitis PDFIstigfarani InBelum ada peringkat
- Nutrition in Islamic PerspectiveDokumen15 halamanNutrition in Islamic PerspectiveRangga Alam VaneoBelum ada peringkat
- "Broken Vow": (Chorus:)Dokumen2 halaman"Broken Vow": (Chorus:)Rangga Alam VaneoBelum ada peringkat
- A e D FDokumen2 halamanA e D FRangga Alam VaneoBelum ada peringkat
- CLONING (Compatibility Mode)Dokumen35 halamanCLONING (Compatibility Mode)Lutfi Aulia SupriyadiBelum ada peringkat
- Dr. Joko Wahyu Wibowo MkesDokumen51 halamanDr. Joko Wahyu Wibowo MkesRangga Alam VaneoBelum ada peringkat
- Untitled 3Dokumen1 halamanUntitled 3Rangga Alam VaneoBelum ada peringkat
- Online Music Courses With NifaDokumen5 halamanOnline Music Courses With NifagksamuraiBelum ada peringkat
- Alpha Phi Omega National Service Fraternity Strategic PlanDokumen1 halamanAlpha Phi Omega National Service Fraternity Strategic Planlafay3tteBelum ada peringkat
- Expected OutcomesDokumen4 halamanExpected OutcomesPankaj MahantaBelum ada peringkat
- Twitch V CruzzControl CreatineOverdoseDokumen19 halamanTwitch V CruzzControl CreatineOverdoseAndy ChalkBelum ada peringkat
- Chapter 1Dokumen2 halamanChapter 1Nor-man KusainBelum ada peringkat
- Diferencias Gas LP y Gas Natural: Adminigas, S.A. de C.VDokumen2 halamanDiferencias Gas LP y Gas Natural: Adminigas, S.A. de C.VMarco Antonio Zelada HurtadoBelum ada peringkat
- Conservation of Kuttichira SettlementDokumen145 halamanConservation of Kuttichira SettlementSumayya Kareem100% (1)
- Opamp TIDokumen5 halamanOpamp TIAmogh Gajaré100% (1)
- Marketing of Agriculture InputsDokumen18 halamanMarketing of Agriculture InputsChanakyaBelum ada peringkat
- Cuplock Scaffold 18mPHx1.6mx2.5m SafetyDokumen1 halamanCuplock Scaffold 18mPHx1.6mx2.5m SafetyDIGITAL SIRBelum ada peringkat
- JTIL Purchase Requisition for Plasma Machine SparesDokumen3 halamanJTIL Purchase Requisition for Plasma Machine Sparesshivam soniBelum ada peringkat
- 6a. ICMR STSDokumen15 halaman6a. ICMR STSVishnu Praba ABelum ada peringkat
- Efficient Power Supply for Inductive LoadsDokumen7 halamanEfficient Power Supply for Inductive LoadsMary AndersonBelum ada peringkat
- Batool2019 Article ANanocompositePreparedFromMagn PDFDokumen10 halamanBatool2019 Article ANanocompositePreparedFromMagn PDFmazharBelum ada peringkat
- EGMM - Training Partner MOUDokumen32 halamanEGMM - Training Partner MOUShaik HussainBelum ada peringkat
- Irc SP 65-2005 PDFDokumen32 halamanIrc SP 65-2005 PDFAjay Kumar JainBelum ada peringkat
- Yardi Commercial SuiteDokumen52 halamanYardi Commercial SuiteSpicyBelum ada peringkat
- SWOT AnalysisDokumen6 halamanSWOT Analysishananshahid96Belum ada peringkat
- Arcelor Mittal - Bridges PDFDokumen52 halamanArcelor Mittal - Bridges PDFShamaBelum ada peringkat
- Solution of Introduction To Many-Body Quantum Theory in Condensed Matter Physics (H.Bruus & K. Flensberg)Dokumen54 halamanSolution of Introduction To Many-Body Quantum Theory in Condensed Matter Physics (H.Bruus & K. Flensberg)Calamanciuc Mihai MadalinBelum ada peringkat
- IBM Systems Journal PerspectivesDokumen24 halamanIBM Systems Journal PerspectivesSmitha MathewBelum ada peringkat
- Fi 7160Dokumen2 halamanFi 7160maxis2022Belum ada peringkat
- Foundry Technology GuideDokumen34 halamanFoundry Technology GuidePranav Pandey100% (1)
- A. What Is Balanced/objective Review or Criticism?Dokumen11 halamanA. What Is Balanced/objective Review or Criticism?Risha Ann CortesBelum ada peringkat
- Bosch Committed to Outsourcing to Boost CompetitivenessDokumen4 halamanBosch Committed to Outsourcing to Boost CompetitivenessPriya DubeyBelum ada peringkat
- Surveying 2 Practical 3Dokumen15 halamanSurveying 2 Practical 3Huzefa AliBelum ada peringkat
- Location: Connectivity To The MuseumDokumen7 halamanLocation: Connectivity To The MuseumAbhishek AjayBelum ada peringkat
- Evolution BrochureDokumen4 halamanEvolution Brochurelucas28031978Belum ada peringkat
- Eating and HealingDokumen19 halamanEating and HealingMariana CoriaBelum ada peringkat
- Audi A3 Quick Reference Guide: Adjusting Front SeatsDokumen4 halamanAudi A3 Quick Reference Guide: Adjusting Front SeatsgordonjairoBelum ada peringkat