Anda mungkin juga menyukai
- Dengue Case Management Card 125085 12x6 Zcard DengueDokumen2 halamanDengue Case Management Card 125085 12x6 Zcard DenguejmbobitBelum ada peringkat
- WHO Dengue Classification and Case Management-FlyerDokumen2 halamanWHO Dengue Classification and Case Management-FlyerKathleen DyBelum ada peringkat
- Dengue TreamentDokumen2 halamanDengue TreamentKevin ChanBelum ada peringkat
- CholeraDokumen5 halamanCholerabishnu011978Belum ada peringkat
- Case Presentation OngDokumen12 halamanCase Presentation OngRaja Azman Raja AhmadBelum ada peringkat
- Upper GI BleedDokumen50 halamanUpper GI BleedNiladri BanerjeeBelum ada peringkat
- Dengue Update: Gan Kai XinDokumen40 halamanDengue Update: Gan Kai XinKai XinBelum ada peringkat
- Managing Severe Capecitabine DiarrhoeaDokumen5 halamanManaging Severe Capecitabine DiarrhoeaJUAN SEBASTIA RIVERA VILLAMIZARBelum ada peringkat
- Management of Acute PancreatitisDokumen31 halamanManagement of Acute PancreatitisLance sorianoBelum ada peringkat
- Hema Case 2Dokumen55 halamanHema Case 2jlcocm-2022-00028Belum ada peringkat
- Lapjag Bangsal IPD 22 OKTOBER DHFDokumen57 halamanLapjag Bangsal IPD 22 OKTOBER DHFLeony Nerry SabatiniBelum ada peringkat
- IV Fluid TherapyDokumen28 halamanIV Fluid TherapyJacinta MaryBelum ada peringkat
- Discharge Plan and RRLDokumen2 halamanDischarge Plan and RRLnicoleBelum ada peringkat
- 79 - Dengue and Dengue Shock SyndromeDokumen5 halaman79 - Dengue and Dengue Shock SyndromeCeejhay Lee0% (1)
- D231: Medical & Surgical Nursing Lecture On GASTROINTESTINAL (GI) BLEEDINGDokumen37 halamanD231: Medical & Surgical Nursing Lecture On GASTROINTESTINAL (GI) BLEEDINGAnamul MasumBelum ada peringkat
- Fulminant Hepatic Failure: 7 October 2009 Morning Report Christine Williams, MDDokumen25 halamanFulminant Hepatic Failure: 7 October 2009 Morning Report Christine Williams, MDAndreas SichoneBelum ada peringkat
- Epoetin AlfaDokumen3 halamanEpoetin Alfaapi-3797941Belum ada peringkat
- Malaria Other ComplicationsDokumen36 halamanMalaria Other ComplicationsmaircusBelum ada peringkat
- Infectious Disease ReviewDokumen12 halamanInfectious Disease ReviewjyothiBelum ada peringkat
- Manage Upper GI Bleed in 33yo Hotel ReceptionistDokumen42 halamanManage Upper GI Bleed in 33yo Hotel ReceptionistMuhammad Naveed AslamBelum ada peringkat
- Upper and Lower Gastrointestinal BleedingDokumen36 halamanUpper and Lower Gastrointestinal BleedingDr. Shatdal Chaudhary100% (2)
- Blood Components and Blood TransfusionDokumen38 halamanBlood Components and Blood TransfusionjosephBelum ada peringkat
- Acute Kidney Injury:: A Brief OutlineDokumen48 halamanAcute Kidney Injury:: A Brief OutlinehanaBelum ada peringkat
- Approach To A Patient With Acute Kidney InjuryDokumen70 halamanApproach To A Patient With Acute Kidney InjuryShivamBelum ada peringkat
- Journal Club Meeting: DR Isha Bansal Moderator: DR Amol DahaleDokumen20 halamanJournal Club Meeting: DR Isha Bansal Moderator: DR Amol DahaleIsha BansalBelum ada peringkat
- Dengue FinalDokumen44 halamanDengue FinalAniket MuleBelum ada peringkat
- Upper Gi BleedDokumen47 halamanUpper Gi BleedAtul SharmaBelum ada peringkat
- Renal Emergency RevisiDokumen103 halamanRenal Emergency Revisidesy f sarahBelum ada peringkat
- Management Dengue HXDokumen6 halamanManagement Dengue HXMalshika JayatissaBelum ada peringkat
- DENGUE Clinician GuideDokumen8 halamanDENGUE Clinician GuideLuis Alfredo LaraBelum ada peringkat
- Managing Upper GI BleedingDokumen20 halamanManaging Upper GI BleedingMoses Jr KazevuBelum ada peringkat
- Dengue - IV Fluid PrinciplesDokumen25 halamanDengue - IV Fluid PrinciplesArjuna BuduhBelum ada peringkat
- IM Case ReportDokumen5 halamanIM Case ReportGurungSurajBelum ada peringkat
- Hypertension FamcoDokumen42 halamanHypertension FamcoMusleh Al MusalhiBelum ada peringkat
- HepatitisDokumen41 halamanHepatitisAli Nawaz khanBelum ada peringkat
- Dengue Fever - Ang Ban HongDokumen46 halamanDengue Fever - Ang Ban HongSharimanfadhly YahayaBelum ada peringkat
- Case Concept Acute PrancreatitisDokumen8 halamanCase Concept Acute PrancreatitisGio GallegoBelum ada peringkat
- Case PresentationDokumen22 halamanCase PresentationVikaBelum ada peringkat
- Age CPGDokumen9 halamanAge CPGSLIBelum ada peringkat
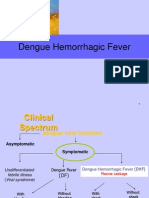
- Dengue Hemorrhagic FeverDokumen27 halamanDengue Hemorrhagic FeverTristiana DewiBelum ada peringkat
- Atul Sharma Uppergi Fcccm23Dokumen47 halamanAtul Sharma Uppergi Fcccm23Atul SharmaBelum ada peringkat
- Managing CKD: regular assessments, BP control, cardiovascular protectionDokumen2 halamanManaging CKD: regular assessments, BP control, cardiovascular protectionRifky Octavio PBelum ada peringkat
- Management Severe DengueDokumen18 halamanManagement Severe DengueMuhammad Fhandeka IsrarBelum ada peringkat
- Essential facts about anemia in pregnancyDokumen40 halamanEssential facts about anemia in pregnancyraph faith100% (1)
- Gastrointestinal HaemorrhageDokumen58 halamanGastrointestinal HaemorrhageAhmed ElwassiefBelum ada peringkat
- Dengue: Denggoy, Dengvaxia, Dengue Ba Sya?Dokumen55 halamanDengue: Denggoy, Dengvaxia, Dengue Ba Sya?KatBelum ada peringkat
- Gi BleedDokumen33 halamanGi BleedMuhammad ArmghanBelum ada peringkat
- Blood Transfusion: Teoman SOYSAL Prof. MDDokumen38 halamanBlood Transfusion: Teoman SOYSAL Prof. MDirdinamarchsyaBelum ada peringkat
- BT New TemplateDokumen65 halamanBT New TemplateNikky SilvestreBelum ada peringkat
- אלון קלציום חלק 3Dokumen25 halamanאלון קלציום חלק 3Alon GoldfainerBelum ada peringkat
- Duty Report Details Woman's Medical IssuesDokumen24 halamanDuty Report Details Woman's Medical IssuesKarina Pratiwi SoetomoBelum ada peringkat
- Aedes aegypti Mosquito and Dengue VirusDokumen34 halamanAedes aegypti Mosquito and Dengue VirusMark ReyesBelum ada peringkat
- Blood TransfusionDokumen32 halamanBlood TransfusionDrPreeti Thakur ChouhanBelum ada peringkat
- CLINICAL ASPECTS OF BLOOD TRANSFUSIONDokumen37 halamanCLINICAL ASPECTS OF BLOOD TRANSFUSIONRaras P P100% (1)
- AHTR Acute Hemolytic Transfusion Reaction Symptoms Causes ManagementDokumen5 halamanAHTR Acute Hemolytic Transfusion Reaction Symptoms Causes ManagementInatrinBelum ada peringkat
- Integrated Pest ManagementDokumen3 halamanIntegrated Pest ManagementMuhammad Luthfi TaufikBelum ada peringkat
- PR DR 4Dokumen21 halamanPR DR 4Muhammad Luthfi TaufikBelum ada peringkat
- Massage Features Within Ancient Indian Ayurvedic Texts Dating Back Over 4Dokumen2 halamanMassage Features Within Ancient Indian Ayurvedic Texts Dating Back Over 4Muhammad Luthfi TaufikBelum ada peringkat
- Are You Interested in ScienceDokumen1 halamanAre You Interested in ScienceMuhammad Luthfi TaufikBelum ada peringkat
- Massage Features Within Ancient Indian Ayurvedic Texts Dating Back Over 4Dokumen2 halamanMassage Features Within Ancient Indian Ayurvedic Texts Dating Back Over 4Muhammad Luthfi TaufikBelum ada peringkat
- Blood and Cardiovascular SystemDokumen7 halamanBlood and Cardiovascular SystemMuhammad Luthfi TaufikBelum ada peringkat
- The Relativistic Brain by Ronald Cicurel and Miguel L. Nicolelis (2015)Dokumen5 halamanThe Relativistic Brain by Ronald Cicurel and Miguel L. Nicolelis (2015)Sinem SerapBelum ada peringkat
- Blue Book PediatricsDokumen126 halamanBlue Book PediatricsKoricho Mengistu100% (1)
- HeparinDokumen2 halamanHeparinNinoska Garcia-Ortiz100% (4)
- Lesson 6 - Musculoskeletal and Nervous SystemsDokumen20 halamanLesson 6 - Musculoskeletal and Nervous Systemsapi-307592530Belum ada peringkat
- Tetralogy of Fallot Everything You Wanted To Know But Were Afraid To AskDokumen8 halamanTetralogy of Fallot Everything You Wanted To Know But Were Afraid To AsksofiaBelum ada peringkat
- Pathogenesis of AtherosclerosisDokumen21 halamanPathogenesis of Atherosclerosishakky gamyBelum ada peringkat
- Risk For Decreased Cardiac OutputDokumen4 halamanRisk For Decreased Cardiac Outputapi-283482759Belum ada peringkat
- Chapter 3: Movement of Substance Across The Plasma MembraneDokumen13 halamanChapter 3: Movement of Substance Across The Plasma MembraneEma FatimahBelum ada peringkat
- 12 SexualQigongDokumen6 halaman12 SexualQigongAnonymous r84IzwCBelum ada peringkat
- Seed Germination, Dormancy & Breaking of DormancyDokumen35 halamanSeed Germination, Dormancy & Breaking of DormancySaravananBelum ada peringkat
- Anesthesiology Resident Survival Guide 2014-2015Dokumen32 halamanAnesthesiology Resident Survival Guide 2014-2015Karla Matos100% (1)
- Paragraph Development ExerciseDokumen6 halamanParagraph Development ExerciseSYAFINAS SALAM100% (1)
- Point MarmaDokumen2 halamanPoint MarmaAnonymous yzbnd8Belum ada peringkat
- Abbreviation For ChartingDokumen12 halamanAbbreviation For ChartingJomar De BelenBelum ada peringkat
- Chapter 4Dokumen7 halamanChapter 4R LashBelum ada peringkat
- Lim Et Al 2017 PDFDokumen37 halamanLim Et Al 2017 PDFkirshBelum ada peringkat
- NCP of CavDokumen3 halamanNCP of CavHenry Roque TagalagBelum ada peringkat
- Biology #KautilyaDokumen79 halamanBiology #KautilyapankajBelum ada peringkat
- Vacuole FunctionDokumen8 halamanVacuole Functionkbansal981Belum ada peringkat
- 3.03 Understand Structures, Functions and Disorders of The Nervous SystemDokumen38 halaman3.03 Understand Structures, Functions and Disorders of The Nervous SystemLoriwinchesterBelum ada peringkat
- Journal Reading Radiologi EllaDokumen44 halamanJournal Reading Radiologi EllaElla Putri SaptariBelum ada peringkat
- Nutrition in Plants and AnimalsDokumen3 halamanNutrition in Plants and AnimalsHaris Ur RehmanBelum ada peringkat
- USABO 17 Open Exam - Final.webDokumen16 halamanUSABO 17 Open Exam - Final.webJ.Chang ChangBelum ada peringkat
- CM All Compiled NotesDokumen100 halamanCM All Compiled NotesKatrina Mae PatalinghugBelum ada peringkat
- C5 - Metabolism and Enzyme Part 1Dokumen20 halamanC5 - Metabolism and Enzyme Part 1Daniel LohBelum ada peringkat
- Movement Disorders Movement DisordersDokumen32 halamanMovement Disorders Movement Disordersreddyrajiv1526Belum ada peringkat
- 10th BIOLOGY PPT CH. NO. 8Dokumen13 halaman10th BIOLOGY PPT CH. NO. 8Aastha BorhadeBelum ada peringkat
- Inguinal CanalDokumen4 halamanInguinal CanalspiraldaoBelum ada peringkat
- Francisco Aboitiz (Auth.) - A Brain For Speech - A View From Evolutionary Neuroanatomy-Palgrave Macmillan UK (2017)Dokumen515 halamanFrancisco Aboitiz (Auth.) - A Brain For Speech - A View From Evolutionary Neuroanatomy-Palgrave Macmillan UK (2017)TecuitlatlBelum ada peringkat