Anda mungkin juga menyukai
- Diabetic Ketoacidosis (DKA)Dokumen33 halamanDiabetic Ketoacidosis (DKA)Eric Chye Teck100% (1)
- Diabetic KetoacidosisDokumen38 halamanDiabetic KetoacidosisAwatef AbushhiwaBelum ada peringkat
- Diabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiDokumen23 halamanDiabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiSreekrishnan Trikkur100% (2)
- 14.malabsorption SyndromesDokumen5 halaman14.malabsorption SyndromesPriyaBelum ada peringkat
- HyperkalemiaDokumen3 halamanHyperkalemiaSergeiBelum ada peringkat
- Diabetes InsipidusDokumen21 halamanDiabetes InsipidusMoni RethBelum ada peringkat
- Different Iv FluidsDokumen2 halamanDifferent Iv FluidsBeverly DatuBelum ada peringkat
- Diabetic Ketoacidosis (Dka)Dokumen18 halamanDiabetic Ketoacidosis (Dka)dr.Bobi Ahmad Sahid, S.Kep100% (2)
- DkaDokumen83 halamanDkaRajaKumar Ponnana100% (1)
- Urine FormationDokumen14 halamanUrine FormationWaziri MbarukuBelum ada peringkat
- 03-07 Lecture Coronary CirculationDokumen29 halaman03-07 Lecture Coronary Circulationaspalavista50% (2)
- Patient ProfileDokumen9 halamanPatient ProfileValarmathiBelum ada peringkat
- Diabetic KetoacidosisDokumen3 halamanDiabetic KetoacidosisJanna FavilaBelum ada peringkat
- Diabetic KetoacidosisDokumen76 halamanDiabetic Ketoacidosisniyigok100% (1)
- Family Case Study For HydrocephalusDokumen9 halamanFamily Case Study For HydrocephalusjaegergranBelum ada peringkat
- Diabetic KetoacidosisDokumen6 halamanDiabetic KetoacidosisRain Catan Gagarra Saquin100% (1)
- Angina PectorisDokumen30 halamanAngina PectorisTaufik Ramadhan Biya83% (6)
- Case Study: Diabetic KetoacidosisDokumen66 halamanCase Study: Diabetic Ketoacidosisllaychin100% (2)
- DKADokumen64 halamanDKAAravindhan Gunasekaran PaediatricianBelum ada peringkat
- Diabetic KetoacidosisDokumen16 halamanDiabetic Ketoacidosisjoyshe111100% (2)
- Pathophysiology of Diabetes MellitusDokumen2 halamanPathophysiology of Diabetes MellitusJerene67% (3)
- LPD - Myrin P Forte (Pakistan)Dokumen17 halamanLPD - Myrin P Forte (Pakistan)Azeem Abbas0% (1)
- Diabetic Ketoacidosis (Dka)Dokumen16 halamanDiabetic Ketoacidosis (Dka)yazid100% (5)
- Addison's DiseaseDokumen15 halamanAddison's DiseaseRonald A. Ogania50% (4)
- Diabetes MellitusDokumen9 halamanDiabetes MellitusM. Joyce100% (2)
- Diabetic Ketoacidosis Written ReportDokumen19 halamanDiabetic Ketoacidosis Written ReportEros Victorino100% (2)
- Case Study 18Dokumen4 halamanCase Study 18api-271284613Belum ada peringkat
- 12a Diabetic Emergencies DKA Case StudiesDokumen13 halaman12a Diabetic Emergencies DKA Case StudiesAnonymous yTdBi7100% (1)
- Chronic Liver DiseaseDokumen12 halamanChronic Liver DiseaseamitBelum ada peringkat
- Physiology of GIT (2) (Autosaved)Dokumen67 halamanPhysiology of GIT (2) (Autosaved)RISALATUL KHOIROTUNISABelum ada peringkat
- Chronic Renal FailureDokumen37 halamanChronic Renal Failuredorkiebaby100% (10)
- Drugs - Icu (Group)Dokumen7 halamanDrugs - Icu (Group)Patricia LuceroBelum ada peringkat
- Physiological Changes During Pregnancy: Presented By: Ms. Vruti PatelDokumen44 halamanPhysiological Changes During Pregnancy: Presented By: Ms. Vruti PatelSANJEEV KUMARBelum ada peringkat
- Renal CalculiDokumen10 halamanRenal CalculiHarpreet Singh100% (1)
- Nursing Management of Patient With CCFDokumen34 halamanNursing Management of Patient With CCFJayarani Ashok100% (1)
- Renal Replacement Therapies Hemodialysis and Peritoneal DialysisDokumen86 halamanRenal Replacement Therapies Hemodialysis and Peritoneal DialysisSabita Tripathi100% (2)
- CS Diabetic KetoacidosisDokumen11 halamanCS Diabetic KetoacidosisMarvin Dela CruzBelum ada peringkat
- CNN Practice QuestionsDokumen5 halamanCNN Practice QuestionsUri Perez MontedeRamosBelum ada peringkat
- Case Presentation: Alcoholic GastritisDokumen18 halamanCase Presentation: Alcoholic Gastritisstancy thomas100% (1)
- Diabetic Ketoacidosis Case PresentationDokumen37 halamanDiabetic Ketoacidosis Case PresentationNathan Vince Cruz100% (2)
- Congestive Cardiac FailureDokumen49 halamanCongestive Cardiac FailureHampson MalekanoBelum ada peringkat
- Nursing Care Plan For Diabetes Mellitus Diabetic KetoacidosisDokumen17 halamanNursing Care Plan For Diabetes Mellitus Diabetic KetoacidosisJordz Placi100% (2)
- Diabetic Ketoacidosis Case StudyDokumen5 halamanDiabetic Ketoacidosis Case Studyjc_albano29100% (7)
- Case Presentation On Chronic Kidney Disease1Dokumen18 halamanCase Presentation On Chronic Kidney Disease1d100% (1)
- Fluid Electrolyte ImbalanceDokumen46 halamanFluid Electrolyte ImbalanceAxsa Alex100% (1)
- DCLDDokumen36 halamanDCLDAnonymous uoxEU3mkBelum ada peringkat
- CVA Case PresentationDokumen25 halamanCVA Case PresentationChucky VergaraBelum ada peringkat
- Diabetic Ketoacidosis (DKA) VS. Hyperosmolar Hyperglycemic Syndrome (HHS)Dokumen5 halamanDiabetic Ketoacidosis (DKA) VS. Hyperosmolar Hyperglycemic Syndrome (HHS)MrRightBelum ada peringkat
- Acute Renal FailureDokumen34 halamanAcute Renal Failureaibaloca67% (9)
- Anemia 130809044630 Phpapp01Dokumen21 halamanAnemia 130809044630 Phpapp01Siddharth Das100% (1)
- Dka Case StudyDokumen3 halamanDka Case StudyMaryjoy Gabriellee De La CruzBelum ada peringkat
- HYPERTENSIONDokumen11 halamanHYPERTENSIONGargiBelum ada peringkat
- Case Study HyperkalemiaDokumen10 halamanCase Study HyperkalemiaJamaica Cerrero100% (1)
- Pass Critical Care Endocrine Frcem ResourcesDokumen41 halamanPass Critical Care Endocrine Frcem ResourcesYoussef SaadBelum ada peringkat
- Diabetic Ketoacidosis (DKA) - Presentation Slide EditedDokumen22 halamanDiabetic Ketoacidosis (DKA) - Presentation Slide EditedTerence Chin0% (1)
- Diabetic EmergenciesDokumen65 halamanDiabetic EmergenciesManmeet SBelum ada peringkat
- Revised DKA 2015 PDFDokumen6 halamanRevised DKA 2015 PDFDr AhmedBelum ada peringkat
- Diabetic KetoacidosisDokumen22 halamanDiabetic KetoacidosismartinBelum ada peringkat
- Somchodok Chakreeyarat, MD. Endocrine Unit, Department of Medicine Bhumibol Adulyadej HospitalDokumen53 halamanSomchodok Chakreeyarat, MD. Endocrine Unit, Department of Medicine Bhumibol Adulyadej HospitalLing TaerahkunBelum ada peringkat
- Abortion: Renhe Hospital Wang JunjieDokumen51 halamanAbortion: Renhe Hospital Wang JunjieMadhu Sudhan PandeyaBelum ada peringkat
- Quick Guide For Candidates: Step 1: Creating An Account and Logging in Create An AccountDokumen2 halamanQuick Guide For Candidates: Step 1: Creating An Account and Logging in Create An AccountMadhu Sudhan Pandeya100% (1)
- Voter ListDokumen214 halamanVoter ListMadhu Sudhan PandeyaBelum ada peringkat
- श्रम एेन २०७४Dokumen53 halamanश्रम एेन २०७४PradIpta Kaphle0% (1)
- Nepal Medical Council Act, 2020 (1964)Dokumen20 halamanNepal Medical Council Act, 2020 (1964)Madhu Sudhan PandeyaBelum ada peringkat
- Who Rights Roles Respon HW Covid 19Dokumen3 halamanWho Rights Roles Respon HW Covid 19HarryBelum ada peringkat
- Lecture-33 Postpartum HemorrhageDokumen50 halamanLecture-33 Postpartum HemorrhageMadhu Sudhan Pandeya100% (2)
- Teratology & Chronic PoisoningDokumen54 halamanTeratology & Chronic PoisoningMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-11 Breech PresentationDokumen27 halamanLecture-11 Breech PresentationMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-28 Placenta PreviaDokumen43 halamanLecture-28 Placenta PreviaMadhu Sudhan Pandeya100% (1)
- Vaccination Guideline: International Travel and Health 2007Dokumen9 halamanVaccination Guideline: International Travel and Health 2007Madhu Sudhan PandeyaBelum ada peringkat
- Lecture-18 Obstructed LaborDokumen8 halamanLecture-18 Obstructed LaborMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-31 Instrumental DeliveryDokumen33 halamanLecture-31 Instrumental DeliveryMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-35 Eectronic Fetal MonitoringDokumen45 halamanLecture-35 Eectronic Fetal MonitoringMadhu Sudhan PandeyaBelum ada peringkat
- Bishop's Pre-Induction Cervical Scoring SystemDokumen2 halamanBishop's Pre-Induction Cervical Scoring SystemMadhu Sudhan PandeyaBelum ada peringkat
- Postpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinDokumen98 halamanPostpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinMadhu Sudhan PandeyaBelum ada peringkat
- Fetal DistressDokumen32 halamanFetal DistressMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-22 Prolonged PregnancyDokumen24 halamanLecture-22 Prolonged PregnancyMadhu Sudhan PandeyaBelum ada peringkat
- Lecture 30 PromDokumen7 halamanLecture 30 PromMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-25 Cesarean SectionDokumen21 halamanLecture-25 Cesarean SectionMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-26 Hypertensive Disease of PregnancyDokumen28 halamanLecture-26 Hypertensive Disease of PregnancyMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-13 Transeverse LieDokumen15 halamanLecture-13 Transeverse LieMadhu Sudhan PandeyaBelum ada peringkat
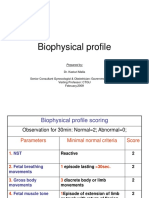
- Lecture-23 Biophysical ProfieDokumen3 halamanLecture-23 Biophysical ProfieMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-17 Shoulder DystociaDokumen20 halamanLecture-17 Shoulder DystociaMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-27 Ectopic PregnancyDokumen38 halamanLecture-27 Ectopic PregnancyMadhu Sudhan PandeyaBelum ada peringkat
- Cord ProlapseDokumen7 halamanCord ProlapseMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-12 Face PresentationDokumen9 halamanLecture-12 Face PresentationMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-6 Obstetric TerminologiesDokumen17 halamanLecture-6 Obstetric TerminologiesMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-15 Prolonged LaborDokumen8 halamanLecture-15 Prolonged LaborMadhu Sudhan PandeyaBelum ada peringkat
- Lecture-24 Twins PregnancyDokumen30 halamanLecture-24 Twins PregnancyMadhu Sudhan PandeyaBelum ada peringkat
- AtacandDokumen30 halamanAtacandAnna KowalskaBelum ada peringkat
- Cardiac RehabilitationDokumen28 halamanCardiac Rehabilitationshivalingam20Belum ada peringkat
- Clinical SignificanceDokumen31 halamanClinical Significancejav israelBelum ada peringkat
- Disorders of Pigmentation 1Dokumen56 halamanDisorders of Pigmentation 1Ahmed Noureldin AhmedBelum ada peringkat
- TR-AUTOHEMOTHERAPY AUTOLOGOUS BLOOD TRANSFUSION OZONE THERAPY Â AN UPDATEDokumen43 halamanTR-AUTOHEMOTHERAPY AUTOLOGOUS BLOOD TRANSFUSION OZONE THERAPY Â AN UPDATEweb3351100% (1)
- Case 25-2020: A 47-Year-Old Woman With A Lung Mass: Case Records Massachusetts General HospitalDokumen10 halamanCase 25-2020: A 47-Year-Old Woman With A Lung Mass: Case Records Massachusetts General HospitalClinica CorominasBelum ada peringkat
- PDF The Biology of Cancer DDDokumen21 halamanPDF The Biology of Cancer DDLunactic ThanosBelum ada peringkat
- SOAPM Alfonso GiulianiDokumen2 halamanSOAPM Alfonso GiulianiEric YoungBelum ada peringkat
- Behavioral Health Care PlanDokumen13 halamanBehavioral Health Care Planapi-521003884Belum ada peringkat
- Rheumatology NotesDokumen10 halamanRheumatology NotesBrandonRyanF.MosidinBelum ada peringkat
- Clinical Practice Guidelines 2021 - Egyptian ORL Society... - Copy-1-185Dokumen185 halamanClinical Practice Guidelines 2021 - Egyptian ORL Society... - Copy-1-185abdalla materBelum ada peringkat
- تجميعات غادة لشهر MayDokumen89 halamanتجميعات غادة لشهر MayMohamed OsamaBelum ada peringkat
- RBC Morphology and InclusionsDokumen3 halamanRBC Morphology and InclusionsDeomicah SolanoBelum ada peringkat
- Surgery (I) Log BookDokumen133 halamanSurgery (I) Log BookQasim HaleimiBelum ada peringkat
- Shannon Hanchett Autopsy ReportDokumen1 halamanShannon Hanchett Autopsy ReportOKCFOXBelum ada peringkat
- Radiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadDokumen100 halamanRadiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadDiana OCtavinaBelum ada peringkat
- Fournier'S Gangrene: Rajah Amina SuleimanDokumen27 halamanFournier'S Gangrene: Rajah Amina SuleimanAmina RajahBelum ada peringkat
- Kubba 2001 (Intervention For Recurren Idiopathix Epistaksis in ChildrenDokumen26 halamanKubba 2001 (Intervention For Recurren Idiopathix Epistaksis in ChildrenRaudhah SimahateBelum ada peringkat
- Towards Better Patient Care Drugs To Avoid in 2024Dokumen11 halamanTowards Better Patient Care Drugs To Avoid in 2024Juan Diego Sánchez BaenaBelum ada peringkat
- CHANCROIDDokumen13 halamanCHANCROIDPradeep YarasaniBelum ada peringkat
- 21.neural Control and CoordinationDokumen44 halaman21.neural Control and Coordinationg1307Belum ada peringkat
- Anatomo-Physiological Peculiarities of The Respiratory System. Percussion of The Lungs.Dokumen40 halamanAnatomo-Physiological Peculiarities of The Respiratory System. Percussion of The Lungs.Hetvi PatelBelum ada peringkat
- Pre-Op Case Protocol #4Dokumen2 halamanPre-Op Case Protocol #4IC BBelum ada peringkat
- SAAI Protocol KankerDokumen4 halamanSAAI Protocol KankerSadha MahardhikaBelum ada peringkat
- GlomerulonephritisDokumen35 halamanGlomerulonephritisapi-19916399Belum ada peringkat
- Solution Manual For Mcgraw Hill Connect Resources For Jones Acquiring Medical Language 1eDokumen58 halamanSolution Manual For Mcgraw Hill Connect Resources For Jones Acquiring Medical Language 1ethomaslucasikwjeqyonm100% (30)
- Need Motivates The Behaviour of A Person.: Human Needs TheoryDokumen8 halamanNeed Motivates The Behaviour of A Person.: Human Needs TheoryDan Ataniel EnsaladaBelum ada peringkat
- Daftar Pustaka: Universitas Sumatera UtaraDokumen4 halamanDaftar Pustaka: Universitas Sumatera Utaraoriza novitaBelum ada peringkat
- CH 32Dokumen6 halamanCH 32Gabriel GonzagaBelum ada peringkat
- Testicular TorsionDokumen20 halamanTesticular TorsionGAURAV100% (3)