Anda mungkin juga menyukai
- Drugs Used in AsthmaDokumen135 halamanDrugs Used in AsthmaDR. MUSICBelum ada peringkat
- Asthma For PTDokumen52 halamanAsthma For PTAnn SibyBelum ada peringkat
- Asma UndanaDokumen36 halamanAsma UndanaNindyBelum ada peringkat
- Anaphylaxis ArticuloDokumen12 halamanAnaphylaxis ArticuloFrancelia Quiñonez RuvalcabaBelum ada peringkat
- B Russell e 2013Dokumen10 halamanB Russell e 2013Arief Janurachman HakimBelum ada peringkat
- Guideline On Management of Asthma in Adult and ChildrenDokumen24 halamanGuideline On Management of Asthma in Adult and ChildrenJerry TanBelum ada peringkat
- Asthma: Rochelle M. Nolte, MD CDR Usphs Family MedicineDokumen56 halamanAsthma: Rochelle M. Nolte, MD CDR Usphs Family MedicineJoan Marie Lechado InoviaBelum ada peringkat
- File 18585Dokumen15 halamanFile 18585Mohammed MuthanaBelum ada peringkat
- Safety of N Acetylcysteine at High Doses in Chronic Respiratory Diseases: A ReviewDokumen18 halamanSafety of N Acetylcysteine at High Doses in Chronic Respiratory Diseases: A Reviewkaroline SernadesBelum ada peringkat
- Asthma 2022Dokumen36 halamanAsthma 2022SePeHR SHBelum ada peringkat
- Astm BronsicDokumen15 halamanAstm BronsicBogdan AdrianaBelum ada peringkat
- Pedia Bronchial Asthma-1Dokumen43 halamanPedia Bronchial Asthma-1MAHEJS HDBelum ada peringkat
- Wireless Sensor Networks in Monitoring of Asthma: Dinko OleticDokumen9 halamanWireless Sensor Networks in Monitoring of Asthma: Dinko OleticShubha ShivaprakashBelum ada peringkat
- Asthma: Review Open AccessDokumen9 halamanAsthma: Review Open AccessKarthik VelletiBelum ada peringkat
- Farmasi Klinis 2 - Asma Akut (Eksaserbasi Asma) - From: Gina 2017 - By: Amelia Lorensia - 2017Dokumen52 halamanFarmasi Klinis 2 - Asma Akut (Eksaserbasi Asma) - From: Gina 2017 - By: Amelia Lorensia - 2017Alifah SyarafinaBelum ada peringkat
- KlasifikasiDokumen8 halamanKlasifikasinurul sachrani putriBelum ada peringkat
- Feno Revision Sistematica Italia 2020Dokumen20 halamanFeno Revision Sistematica Italia 2020Estefania Yu AcevedoBelum ada peringkat
- Doxovent M MedicalDokumen38 halamanDoxovent M MedicalkurutalaBelum ada peringkat
- Editorial: Bronchial Asthma - Issues For The Developing WorldDokumen3 halamanEditorial: Bronchial Asthma - Issues For The Developing WorldHow ToBelum ada peringkat
- Asma 2022 PDFDokumen66 halamanAsma 2022 PDFBagas Trikuncoro BawonoBelum ada peringkat
- Zhu 18 05Dokumen8 halamanZhu 18 05ABBelum ada peringkat
- Asthma Control: Guideline BasedDokumen38 halamanAsthma Control: Guideline BaseddianutamiaBelum ada peringkat
- Asthma Case PresentationDokumen3 halamanAsthma Case Presentationfernandezrachelle44Belum ada peringkat
- Asthma and COPDDokumen74 halamanAsthma and COPDCharles YiuBelum ada peringkat
- Asthma and COPD by AkkoDokumen17 halamanAsthma and COPD by AkkoAvoy GhoshBelum ada peringkat
- Presented By: MANOJ MANDAL 1 Year P.C BSC NSG, Mibe, GSNDokumen42 halamanPresented By: MANOJ MANDAL 1 Year P.C BSC NSG, Mibe, GSNfurr singhBelum ada peringkat
- Adult Nursing - The Final PresentationDokumen70 halamanAdult Nursing - The Final Presentationក្មេងប្រុស ល្ងីល្ងើBelum ada peringkat
- Clinical ManagementDokumen14 halamanClinical ManagementJohn GichunjiBelum ada peringkat
- Asthma Prevention and Control SeminarDokumen17 halamanAsthma Prevention and Control Seminarridwan sanusiBelum ada peringkat
- Clinical Management of AsthmaDokumen14 halamanClinical Management of AsthmaIndah Putriani IbnuBelum ada peringkat
- Bringing Asthma Care Into The Twenty-First Century: Review ArticleDokumen11 halamanBringing Asthma Care Into The Twenty-First Century: Review ArticleliadiafaridaBelum ada peringkat
- Docsbookstoreacsapac2022b1 Sample PDFDokumen30 halamanDocsbookstoreacsapac2022b1 Sample PDFFaheem Mahmood ButtBelum ada peringkat
- Japanese Guidelines For Childhood Asthma 2017 PDFDokumen15 halamanJapanese Guidelines For Childhood Asthma 2017 PDFcindy315Belum ada peringkat
- Asthma: Allergy Asthma and Clinical Immunology November 2011Dokumen10 halamanAsthma: Allergy Asthma and Clinical Immunology November 2011Sarmad AlwardiBelum ada peringkat
- Asthmatic Attack: Miriti M.D Masters of Clinical Medicine Accidents and Emergency Facilitator: DR Simba DR MburuguDokumen26 halamanAsthmatic Attack: Miriti M.D Masters of Clinical Medicine Accidents and Emergency Facilitator: DR Simba DR MburuguDennis MiritiBelum ada peringkat
- Bronchial AsthmaDokumen59 halamanBronchial Asthmashefalika mandremBelum ada peringkat
- Pi Is 1323893016301745Dokumen27 halamanPi Is 1323893016301745Afria TikaBelum ada peringkat
- Asma 2020Dokumen66 halamanAsma 2020sarifullatang laseBelum ada peringkat
- AsthmaDokumen95 halamanAsthmaMohiuddin AhmedBelum ada peringkat
- GP Reg - Asthma and Spirometry 2011Dokumen114 halamanGP Reg - Asthma and Spirometry 2011minerva_stanciuBelum ada peringkat
- Asthma: Chronic Inflammation of The Airways. The Hyper-Responsive Airways Typical of AsthmaDokumen7 halamanAsthma: Chronic Inflammation of The Airways. The Hyper-Responsive Airways Typical of AsthmaRaj PaulBelum ada peringkat
- Respirology 2023 FinalDokumen127 halamanRespirology 2023 FinalBelinda ELISHABelum ada peringkat
- Use of Biologics in AsthmaDokumen55 halamanUse of Biologics in Asthmaosama.khalifaBelum ada peringkat
- NCM 112 Lec 2Dokumen64 halamanNCM 112 Lec 2JIMENEZ, TRISHA MARIE D.Belum ada peringkat
- Asthma: Signs and SymptomsDokumen57 halamanAsthma: Signs and SymptomsAjp Ryuzaki CaesarBelum ada peringkat
- Respiratory Disorder Note BSC 3rd YearDokumen41 halamanRespiratory Disorder Note BSC 3rd YearNancyBelum ada peringkat
- Asma 3Dokumen12 halamanAsma 3nabilla putriBelum ada peringkat
- Iadt 08 S 1 P 713Dokumen12 halamanIadt 08 S 1 P 713Atchiim AifBelum ada peringkat
- Asthma: Practice EssentialsDokumen12 halamanAsthma: Practice EssentialsIda WilonaBelum ada peringkat
- AsthmaDokumen8 halamanAsthmahusainozelBelum ada peringkat
- Jaa 4 001 PDFDokumen12 halamanJaa 4 001 PDFRulianti BarantiBelum ada peringkat
- Icbt 10 I 12 P 1417Dokumen8 halamanIcbt 10 I 12 P 1417Berina ŠarićBelum ada peringkat
- Asthma: Assessment, Diagnosis, and Treatment Adherence: Gerri KaufmanDokumen8 halamanAsthma: Assessment, Diagnosis, and Treatment Adherence: Gerri KaufmandessyBelum ada peringkat
- Cough Freq AsthmaDokumen8 halamanCough Freq AsthmaDiogo TecelãoBelum ada peringkat
- Uncontrolled AsthmaDokumen11 halamanUncontrolled Asthmanac fehBelum ada peringkat
- Asma 2019Dokumen64 halamanAsma 2019ajeng putriBelum ada peringkat
- Asma China 2014Dokumen9 halamanAsma China 2014Diego CedamanosBelum ada peringkat
- Fast Facts: Asthma: Improve patient self-management and drug use, achieve asthma controlDari EverandFast Facts: Asthma: Improve patient self-management and drug use, achieve asthma controlBelum ada peringkat
- Diagnosis and Treatment of Chronic CoughDari EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoBelum ada peringkat
- IMPaCCT EU - Standards For Paediatric Palliative Care in EuropeDokumen8 halamanIMPaCCT EU - Standards For Paediatric Palliative Care in EuropeSaraBelum ada peringkat
- Survey EditedDokumen1 halamanSurvey Editedrobert palomasBelum ada peringkat
- Mini Case Study For MR ADokumen3 halamanMini Case Study For MR Aapi-300133703Belum ada peringkat
- Balanced Scorecard Template 07Dokumen15 halamanBalanced Scorecard Template 07DiyanaBelum ada peringkat
- Reviewer in English 5Dokumen2 halamanReviewer in English 5Christine HernandezBelum ada peringkat
- MCN Lec M1L1 ReviewerDokumen4 halamanMCN Lec M1L1 ReviewerEmily BernatBelum ada peringkat
- Mola Hidantidosa & Gestational Trophoblastic NeoplasmaDokumen23 halamanMola Hidantidosa & Gestational Trophoblastic NeoplasmanurkamilawatiBelum ada peringkat
- Mcqs - Obstetrics and Gynaecology (For Post Graduate Preparing For FNB and Professionals) Obstetrics and GynaecologyDokumen27 halamanMcqs - Obstetrics and Gynaecology (For Post Graduate Preparing For FNB and Professionals) Obstetrics and GynaecologyAnonymous kQCQ30Rq5OBelum ada peringkat
- Reading Comprehension - Food FrightDokumen4 halamanReading Comprehension - Food FrightStephanie RetamarBelum ada peringkat
- Animal Research As A Basis For Clinical Trials: FocusDokumen5 halamanAnimal Research As A Basis For Clinical Trials: FocusIuliana MogaBelum ada peringkat
- Food Science and Nutrition (FSN) - Cal Poly Catalog - FSNDokumen6 halamanFood Science and Nutrition (FSN) - Cal Poly Catalog - FSNmyelkenBelum ada peringkat
- Reading Material - Case - Studies - in - Occupational - Health - and - Safety - ManagementDokumen11 halamanReading Material - Case - Studies - in - Occupational - Health - and - Safety - ManagementJoker KingBelum ada peringkat
- UNICEF Early Childhood COVID-19 Response - 2021Dokumen39 halamanUNICEF Early Childhood COVID-19 Response - 2021Manja125Belum ada peringkat
- Information Booklet 1 PDFDokumen40 halamanInformation Booklet 1 PDFVandana RanaBelum ada peringkat
- Carmen Best Background InformationDokumen15 halamanCarmen Best Background InformationKING 5 NewsBelum ada peringkat
- Sultan Ali Akbar Sinenggayan High School: Program of Activities Activity Target Date Resources Need Expected OutputDokumen5 halamanSultan Ali Akbar Sinenggayan High School: Program of Activities Activity Target Date Resources Need Expected OutputRAHIB SAMAYATINBelum ada peringkat
- 119 FullDokumen14 halaman119 FullClarestaBelum ada peringkat
- Reflection PaperDokumen7 halamanReflection Paperapi-590313144Belum ada peringkat
- Covid WarriorsDokumen103 halamanCovid WarriorsMG Rao100% (1)
- Faktor Resiko Infeksi SCDokumen11 halamanFaktor Resiko Infeksi SCAlberto BrahmBelum ada peringkat
- Hygiene Funda 1 2nd SemDokumen22 halamanHygiene Funda 1 2nd Semlegion alexandersBelum ada peringkat
- Construction Management Plan: Project: Yarra One Apartments 16-22 Claremont Street, South Yarra 3141Dokumen44 halamanConstruction Management Plan: Project: Yarra One Apartments 16-22 Claremont Street, South Yarra 3141Hamdy KarBelum ada peringkat
- Covid-19 Among Neonates: Experience From An Sncu of A Tertiary Care Hospital in Eastern IndiaDokumen4 halamanCovid-19 Among Neonates: Experience From An Sncu of A Tertiary Care Hospital in Eastern IndiaIJAR JOURNALBelum ada peringkat
- Medical Emergencies in Dental Practice: A Review: July 2016Dokumen18 halamanMedical Emergencies in Dental Practice: A Review: July 2016AnushkaBelum ada peringkat
- GHB GBL Chem Sex - Pepse v2Dokumen11 halamanGHB GBL Chem Sex - Pepse v2Luwei ShenBelum ada peringkat
- Mentor Interview Questions TemplateDokumen3 halamanMentor Interview Questions Templateapi-381640393Belum ada peringkat
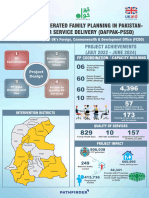
- Poster Sindh 2-01-2024Dokumen11 halamanPoster Sindh 2-01-2024FM Printers111Belum ada peringkat
- Hse Plan 3Dokumen14 halamanHse Plan 3YcRij SeYerBelum ada peringkat
- Agujero MacularDokumen39 halamanAgujero MacularKate CastañoBelum ada peringkat
- Bhutan, Keeping PromisesDokumen44 halamanBhutan, Keeping Promisesstevens106Belum ada peringkat