Anda mungkin juga menyukai
- Schuessler Tissue SaltsDokumen65 halamanSchuessler Tissue Saltsaruen79100% (5)
- TOXICOLOGYDokumen34 halamanTOXICOLOGYBismah Saeed100% (1)
- Poisoning PDFDokumen124 halamanPoisoning PDFDawn WRein Legaspi50% (2)
- Hobart Filler Metals CatalogDokumen244 halamanHobart Filler Metals CatalogBhrugu DhokaiBelum ada peringkat
- DR Kaleem Khan Assistant Professor JNMCHDokumen63 halamanDR Kaleem Khan Assistant Professor JNMCHKaleem KhanBelum ada peringkat
- Tablet Disintegration Test and Basket Rack AssemblyDokumen2 halamanTablet Disintegration Test and Basket Rack AssemblyPhoenix100% (1)
- Critical care approach to poisoned patientsDokumen90 halamanCritical care approach to poisoned patientsGopi KrishnanBelum ada peringkat
- Comprehensive Nclex Notes - Easy To ReadDokumen97 halamanComprehensive Nclex Notes - Easy To ReadBilal Yousuf98% (58)
- Carbo VegetabilisDokumen6 halamanCarbo VegetabilisSuhas IngaleBelum ada peringkat
- Forensic Analysis of Hair EvidenceDokumen29 halamanForensic Analysis of Hair EvidenceEub EuBelum ada peringkat
- Biochemic RemediesDokumen5 halamanBiochemic RemediesJigar PatelBelum ada peringkat
- Penanganan Pertama Keracunan MakananDokumen38 halamanPenanganan Pertama Keracunan Makananony100% (2)
- Phosphorus: Essential Nonmetal Element of LifeDokumen7 halamanPhosphorus: Essential Nonmetal Element of LifeShubhanshi Bhasin100% (1)
- Repair and Rehabilitation of Reinforced ConcreteDokumen15 halamanRepair and Rehabilitation of Reinforced ConcreteebinVettuchirayil100% (2)
- NURSING CARE ON CLIENTS WITH DIARRHEADokumen30 halamanNURSING CARE ON CLIENTS WITH DIARRHEAyustiBelum ada peringkat
- Heavy Metals and Their AntagonistsDokumen42 halamanHeavy Metals and Their AntagonistsMohammad AzharuddinBelum ada peringkat
- Training For Handling Hazardous MaterialsDokumen24 halamanTraining For Handling Hazardous Materialssyreiljude100% (3)
- Hair and Fiber AnalysisDokumen37 halamanHair and Fiber AnalysisKaleem KhanBelum ada peringkat
- FCC Wash Water SystemsDokumen16 halamanFCC Wash Water SystemsBehnam RahzaniBelum ada peringkat
- Effect of Heavy Metals on Oxidative Stress MarkersDokumen6 halamanEffect of Heavy Metals on Oxidative Stress MarkersDesy RusianaBelum ada peringkat
- Introduction To Steam DistributionDokumen6 halamanIntroduction To Steam DistributionKagira Drawing SoltuionBelum ada peringkat
- NCP: Chronic Renal FailureDokumen14 halamanNCP: Chronic Renal FailureJavie77% (13)
- Environmental ToxicologyDokumen10 halamanEnvironmental ToxicologyOmer SyedBelum ada peringkat
- Keracunan Makanan - Dr. SigitDokumen26 halamanKeracunan Makanan - Dr. Sigitfaiza rahmaBelum ada peringkat
- EnviroChem Additional PDFDokumen503 halamanEnviroChem Additional PDFJane PollyBelum ada peringkat
- Arsenic ToxicityDokumen26 halamanArsenic ToxicityDyar MzafarBelum ada peringkat
- Arsenic Poisoning: Causes, Effects, Diagnosis and TreatmentDokumen64 halamanArsenic Poisoning: Causes, Effects, Diagnosis and TreatmentAdarshBijapurBelum ada peringkat
- 8 Environmental Toxicology ATSDR Tox ProfilesDokumen20 halaman8 Environmental Toxicology ATSDR Tox ProfilesAurora Çizmja100% (1)
- Iron Toxic Heavy Metals Fact SheetDokumen1 halamanIron Toxic Heavy Metals Fact SheetosumexBelum ada peringkat
- Metallic PoisonsDokumen29 halamanMetallic PoisonsUjjawalShriwastavBelum ada peringkat
- ARSENICDokumen29 halamanARSENICVatsal RastogiBelum ada peringkat
- Carbolic Acid & Oxalic AcidDokumen46 halamanCarbolic Acid & Oxalic AcidImteaz ahamadBelum ada peringkat
- Arsenic & Copper ModiDokumen32 halamanArsenic & Copper Modikf9tqpnkrzBelum ada peringkat
- A StudyDokumen23 halamanA StudyJames JosephBelum ada peringkat
- ArsenicDokumen11 halamanArsenicShuvashishSunuwarBelum ada peringkat
- ArsenicDokumen16 halamanArsenicKumar DashBelum ada peringkat
- MetalsDokumen113 halamanMetalsمصطفى أحمدBelum ada peringkat
- ToxicologyDokumen9 halamanToxicologyarnav15magicBelum ada peringkat
- Arsenic Poisoning Sources and EffectsDokumen4 halamanArsenic Poisoning Sources and EffectsFreelancer Sanjay TiwariBelum ada peringkat
- ArsenicDokumen27 halamanArsenicDr. Tahir MunirBelum ada peringkat
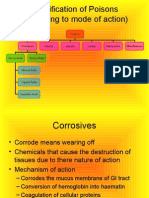
- Classification of Poisons (According To Mode of Action)Dokumen133 halamanClassification of Poisons (According To Mode of Action)dr rizwanBelum ada peringkat
- "Arsenic Poisoning in Animals" EtiologyDokumen4 halaman"Arsenic Poisoning in Animals" Etiologysafi ullahBelum ada peringkat
- Systemic ToxicologyDokumen18 halamanSystemic ToxicologybetsyBelum ada peringkat
- Arsenic Toxicity: Done by // دبع دمحا ءاروح يداهلا بيهو دمحم ءارهز Group ADokumen20 halamanArsenic Toxicity: Done by // دبع دمحا ءاروح يداهلا بيهو دمحم ءارهز Group AIbrahim MohammedBelum ada peringkat
- Corrosive PoisonsDokumen33 halamanCorrosive PoisonsThank MubarakBelum ada peringkat
- Common Poisons 20Dokumen49 halamanCommon Poisons 20ARIF-UR-REHMANBelum ada peringkat
- Sarcodes: The Important Sarcodes Are Adrenalinum Cholesterinum Insulinum Pituitarinum Pepsinum Pancreatinum ThyroidinumDokumen17 halamanSarcodes: The Important Sarcodes Are Adrenalinum Cholesterinum Insulinum Pituitarinum Pepsinum Pancreatinum ThyroidinumMADHURI DHUMAKBelum ada peringkat
- Poisoning in ChildrenDokumen11 halamanPoisoning in ChildrenAndriana HalfienBelum ada peringkat
- A RSENICDokumen34 halamanA RSENICKesavan GnanasekaranBelum ada peringkat
- Pediatri Gawat DaruratDokumen32 halamanPediatri Gawat DaruratAnityo NugrohoBelum ada peringkat
- Cerium: Bonite - Lucero - SevillaDokumen17 halamanCerium: Bonite - Lucero - SevillaGlen Lester ChiongBelum ada peringkat
- PoisoningDokumen52 halamanPoisoninganimesh pandaBelum ada peringkat
- 2 ToxicologyDokumen18 halaman2 Toxicologyنوف الحربي.Belum ada peringkat
- Lecture 06 (Corrosive - Organic Acids) 2Dokumen45 halamanLecture 06 (Corrosive - Organic Acids) 2saraBelum ada peringkat
- PoisoningDokumen39 halamanPoisoningNatnael ShifferawBelum ada peringkat
- Emergency 2Dokumen86 halamanEmergency 2Harley Justiniani Dela CruzBelum ada peringkat
- Everything You Need to Know About Schuessler's Tissue SaltsDokumen7 halamanEverything You Need to Know About Schuessler's Tissue SaltsHMBelum ada peringkat
- Odynophagia Is Painful SwallowingDokumen21 halamanOdynophagia Is Painful SwallowingVien CaagbayBelum ada peringkat
- Dyah Trifianingsih, S. Kep. Ners. M. KepDokumen76 halamanDyah Trifianingsih, S. Kep. Ners. M. KepSiprianus S SBelum ada peringkat
- Toxicology: Saba SaeedDokumen34 halamanToxicology: Saba SaeedMudassir FarooqBelum ada peringkat
- Presenter: Dr. Nishant Shah M.V.Sc. (Medicine)Dokumen104 halamanPresenter: Dr. Nishant Shah M.V.Sc. (Medicine)Santosh BhandariBelum ada peringkat
- Problem 6 KGD: Maria Marcella 405090007Dokumen121 halamanProblem 6 KGD: Maria Marcella 405090007Yessica TheresiaBelum ada peringkat
- Carbolic Aci134Dokumen29 halamanCarbolic Aci13404 Sayali KharadeBelum ada peringkat
- Poisoning in Children: Prepared By, Gayathri R 2 Yr MSC (N)Dokumen124 halamanPoisoning in Children: Prepared By, Gayathri R 2 Yr MSC (N)Gayathri RBelum ada peringkat
- Lithium Carbonate Uses and SymptomsDokumen6 halamanLithium Carbonate Uses and SymptomsSuharikaBelum ada peringkat
- Poisoning in ChildrenDokumen44 halamanPoisoning in ChildrenYohanes FirmansyahBelum ada peringkat
- Unfolding: By: Prof. Dr. Hardik Khamar M.D. (Hom.)Dokumen6 halamanUnfolding: By: Prof. Dr. Hardik Khamar M.D. (Hom.)HomeoDr Babar AminBelum ada peringkat
- Common Indian Plant PoisionsDokumen45 halamanCommon Indian Plant PoisionsRam Kirubakar ThangarajBelum ada peringkat
- 3-Pharynx. OesophagusDokumen30 halaman3-Pharynx. OesophagusislamBelum ada peringkat
- LEGITHMACYDokumen30 halamanLEGITHMACYKaleem KhanBelum ada peringkat
- Transport Accident InjuriesDokumen34 halamanTransport Accident InjuriesKaleem KhanBelum ada peringkat
- EOSIN STAINING ALCOHOL SOLUTION MSDSDokumen11 halamanEOSIN STAINING ALCOHOL SOLUTION MSDSfitrisya luckyBelum ada peringkat
- Chia Seed Paper PDFDokumen7 halamanChia Seed Paper PDFFARCASANU MARIA-ANDREEABelum ada peringkat
- ABB CorrosionDokumen8 halamanABB CorrosionForexFFBelum ada peringkat
- Large-Particle CompositesDokumen25 halamanLarge-Particle CompositesLexBelum ada peringkat
- E 155 - 00 - Rte1nq - PDFDokumen4 halamanE 155 - 00 - Rte1nq - PDFLeón SuárezBelum ada peringkat
- AP Precision Metals BrochureDokumen16 halamanAP Precision Metals Brochureapprecision0% (1)
- Cracks in ConcreteDokumen45 halamanCracks in ConcreteRanjeet SinghBelum ada peringkat
- Crystal Appearance/Characteristics Clinical SignificanceDokumen4 halamanCrystal Appearance/Characteristics Clinical SignificanceAngela LaglivaBelum ada peringkat
- Derouging & Passivation Webinar - Q&A PDFDokumen4 halamanDerouging & Passivation Webinar - Q&A PDFDheeraj Chowdary DhanekulaBelum ada peringkat
- Fiber Optic-Supreme PDFDokumen17 halamanFiber Optic-Supreme PDFdHanE anasBelum ada peringkat
- रासायनिक सूत्र (Chemical Formula) - Padhobeta.com Blog PDFDokumen3 halamanरासायनिक सूत्र (Chemical Formula) - Padhobeta.com Blog PDFRAKISHO WORLDBelum ada peringkat
- Oxynitrox MsdsDokumen4 halamanOxynitrox MsdscapdesuroBelum ada peringkat
- Corian in Healthcare enDokumen8 halamanCorian in Healthcare engoomeshwar9003Belum ada peringkat
- Technical Bulletin: Ammonium Sulfate Solution, 4.1 MDokumen4 halamanTechnical Bulletin: Ammonium Sulfate Solution, 4.1 MToe PaingBelum ada peringkat
- Detailed Chemical Industry Project ProfilesDokumen2 halamanDetailed Chemical Industry Project Profileschirag sabhayaBelum ada peringkat
- Vision IAS Prelims 2020 Test 18 SDokumen34 halamanVision IAS Prelims 2020 Test 18 StriloksinghmeenaBelum ada peringkat
- Set1 Mono-Methylation of H3K4 in S. Cerevisiae Is Advantageous For Survival Under Histidine Starvation Conditions in The Presence of 3-Amino-1,2,4-TriazoleDokumen19 halamanSet1 Mono-Methylation of H3K4 in S. Cerevisiae Is Advantageous For Survival Under Histidine Starvation Conditions in The Presence of 3-Amino-1,2,4-TriazoleAlex GriffithBelum ada peringkat
- Chemical Resistance Chart For AcrylicDokumen2 halamanChemical Resistance Chart For AcrylicNasim KhanBelum ada peringkat
- Battery Basics: Cell Chemistry and DesignDokumen40 halamanBattery Basics: Cell Chemistry and DesignAliBelum ada peringkat
- Boiler OEE Calculation Ver1.00Dokumen29 halamanBoiler OEE Calculation Ver1.00kumarjay36471530100% (1)
- Wang and Helliwell (2001) Determination of Flavonols in Green and Black Tea LeavesDokumen5 halamanWang and Helliwell (2001) Determination of Flavonols in Green and Black Tea LeavesYvonne TongBelum ada peringkat
- History of Hemostasis in Neurosurgery Paulo Et Al 2018Dokumen14 halamanHistory of Hemostasis in Neurosurgery Paulo Et Al 2018AlexBelum ada peringkat
- Process Fluid Mechanics BTech 3rd Sem Mewar UniversityDokumen3 halamanProcess Fluid Mechanics BTech 3rd Sem Mewar UniversityMahboob AlamBelum ada peringkat
- 10 Science Imp Ch3 1Dokumen8 halaman10 Science Imp Ch3 1rajkumar trivediBelum ada peringkat