Anda mungkin juga menyukai
- Anatomy of The Senses QuickStudy Reference Guide - (HEARING)Dokumen2 halamanAnatomy of The Senses QuickStudy Reference Guide - (HEARING)statsoBelum ada peringkat
- Atlas of Human Anatomy - Including Student Consult Interactive Ancillaries and GuidesDokumen11 halamanAtlas of Human Anatomy - Including Student Consult Interactive Ancillaries and GuidesAndrijana StevancevicBelum ada peringkat
- Chapter 8 Lab Assignment - Appendicular Skeleton LabelingDokumen6 halamanChapter 8 Lab Assignment - Appendicular Skeleton Labelingadriana blanco galianoBelum ada peringkat
- Skeletal System ActicityDokumen1 halamanSkeletal System Acticityrozariah mclaughlinBelum ada peringkat
- Fiches AnatomyDokumen6 halamanFiches AnatomyAnas Ismail100% (2)
- Joints Schematic PictureDokumen1 halamanJoints Schematic PictureMOHSEN PMBelum ada peringkat
- Note 17 Nov 2022Dokumen19 halamanNote 17 Nov 2022Raghad RBelum ada peringkat
- Poster01 Skeletal-System-Anterior Ledger11x17Dokumen1 halamanPoster01 Skeletal-System-Anterior Ledger11x17jeffrin alexanderBelum ada peringkat
- Unit VI Powerpoint SlidesDokumen34 halamanUnit VI Powerpoint SlidesSteve Sullivan80% (5)
- PostersDokumen8 halamanPostersVictoria CristobalBelum ada peringkat
- Reviewsheet12Dokumen5 halamanReviewsheet12villafrancatin8Belum ada peringkat
- Kin2222 - Ankle + Foot-1Dokumen27 halamanKin2222 - Ankle + Foot-1AmreenBelum ada peringkat
- Zoo 113 Selected SlidesDokumen29 halamanZoo 113 Selected SlidesSheila Marie CuananBelum ada peringkat
- The Temporomandibular Joints, Teeth, and Muscles, and Their FunctionsDokumen16 halamanThe Temporomandibular Joints, Teeth, and Muscles, and Their Functionsfalop41797Belum ada peringkat
- Resumão, Resumo, Articulações e Ligamentos, Anatomia - Passei DiretoDokumen3 halamanResumão, Resumo, Articulações e Ligamentos, Anatomia - Passei DiretoPablo FranzoniBelum ada peringkat
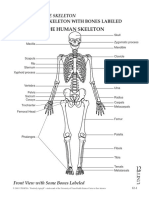
- Bones Teacher Skeleton With Bones Labeled 2ADokumen1 halamanBones Teacher Skeleton With Bones Labeled 2AXenia Marie Razalo LawanBelum ada peringkat
- Bones Teacher Skeleton With Bones Labeled 2A PDFDokumen1 halamanBones Teacher Skeleton With Bones Labeled 2A PDFXenia Marie Razalo LawanBelum ada peringkat
- Diencephalon, Brainstem & CerebellumDokumen1 halamanDiencephalon, Brainstem & CerebellumwinBelum ada peringkat
- ZOOLOGYDokumen3 halamanZOOLOGYJackelyn SalazarBelum ada peringkat
- Poster02 Skeletal-System-Posterior Ledger11x17Dokumen1 halamanPoster02 Skeletal-System-Posterior Ledger11x17jeffrin alexanderBelum ada peringkat
- Sternum PDFDokumen1 halamanSternum PDFKun HanifahBelum ada peringkat
- Bony Framework of Thorax : Anterior ViewDokumen1 halamanBony Framework of Thorax : Anterior ViewKun HanifahBelum ada peringkat
- (Dale Nibbe) Brain Reference Guide PDFDokumen2 halaman(Dale Nibbe) Brain Reference Guide PDFSuryakantaRoulTuntun100% (4)
- 014B - Toad Skeleton - Answer SheetDokumen2 halaman014B - Toad Skeleton - Answer SheetBenjamin James Franklin MaraponBelum ada peringkat
- Frog AtlasDokumen16 halamanFrog AtlasJAYHANNE PSYCHE MONDIABelum ada peringkat
- Diagrams of EyeballDokumen7 halamanDiagrams of EyeballHelworBelum ada peringkat
- Anatomical Landmarks: Here Is Where Your Presentation BeginsDokumen2 halamanAnatomical Landmarks: Here Is Where Your Presentation BeginsAmanda Leigh AquinoBelum ada peringkat
- 7 Special SensesDokumen99 halaman7 Special SensesShaine S. Dimailig0% (1)
- Student Reviewer6Dokumen10 halamanStudent Reviewer6Jessica PalacioBelum ada peringkat
- UntitledDokumen15 halamanUntitledSwitzel Smyle Goh PuyaoanBelum ada peringkat
- NG 1998Dokumen11 halamanNG 1998jovano15Belum ada peringkat
- Buku Ident KepitingDokumen111 halamanBuku Ident KepitingihsanBelum ada peringkat
- Labeled Parts of The Skeletal SystemDokumen37 halamanLabeled Parts of The Skeletal SystemJulienne Ray Hyacinth E. CARVAJALBelum ada peringkat
- Deiuliis2019 VERTEBRADOS LA PERCA 4Dokumen10 halamanDeiuliis2019 VERTEBRADOS LA PERCA 4Fernando Melo GarciaBelum ada peringkat
- EstomihMtuiGreg 2012 CerebralTopography ClinicalNeuroanatomyADokumen23 halamanEstomihMtuiGreg 2012 CerebralTopography ClinicalNeuroanatomyANastya PapounidouBelum ada peringkat
- BI 232 Lab 11Dokumen12 halamanBI 232 Lab 11Cj LinceBelum ada peringkat
- The Skeleton: Chapter 7 Part ADokumen79 halamanThe Skeleton: Chapter 7 Part ADon KeyBelum ada peringkat
- Musculoskeletal Anatomy: Lesson 3: The Structure of Mastication: The Jaws and DentitionDokumen11 halamanMusculoskeletal Anatomy: Lesson 3: The Structure of Mastication: The Jaws and DentitionMarian AlecsBelum ada peringkat
- Facial IsDokumen3 halamanFacial IsSrdjan SekularacBelum ada peringkat
- Anatomi 643Dokumen1 halamanAnatomi 643winBelum ada peringkat
- Dokumen - Pub Laboratory Manual For Anatomy and Physiology 6th Edition 6 978 1119304142 (151 200)Dokumen50 halamanDokumen - Pub Laboratory Manual For Anatomy and Physiology 6th Edition 6 978 1119304142 (151 200)hamria16Belum ada peringkat
- Unit VIIIb Power PointDokumen18 halamanUnit VIIIb Power PointSteve Sullivan100% (3)
- Posterior BonesDokumen1 halamanPosterior BonesRheal P EsmailBelum ada peringkat
- Humerus and Scapula: Posterior View : See Also Plate 183Dokumen1 halamanHumerus and Scapula: Posterior View : See Also Plate 183MihaelaBelum ada peringkat
- General Anatomy - 8Dokumen3 halamanGeneral Anatomy - 8ayaaqassimalmodafarBelum ada peringkat
- NL Parts of The Skeletal SystemDokumen22 halamanNL Parts of The Skeletal SystemJela AgengaBelum ada peringkat
- 11 Bab 4 Sistem Gerak PasifDokumen27 halaman11 Bab 4 Sistem Gerak PasifNurul Ilma Novita Rasyid 9.1Belum ada peringkat
- Cranial Nerves OverviewDokumen18 halamanCranial Nerves OverviewAndrew EldeiryBelum ada peringkat
- Compilation of Netters Illustrations Moores Tables and SnellDokumen50 halamanCompilation of Netters Illustrations Moores Tables and SnellAyres EvangBelum ada peringkat
- Caput Femoriis-Gambar AnatomiiDokumen1 halamanCaput Femoriis-Gambar Anatomiiqonita.jayanti2603Belum ada peringkat
- Pterygopalatine Fossa: Arteries, Veins, and Innervation of The Maxilla and The MandibleDokumen35 halamanPterygopalatine Fossa: Arteries, Veins, and Innervation of The Maxilla and The MandibleFherlee MolinaBelum ada peringkat
- יסמין אוריגין אינסרצין גפייםDokumen36 halamanיסמין אוריגין אינסרצין גפייםmeshi.fishBelum ada peringkat
- Accessory Structures of The Eye: (Photoreceptors) Sense and EyelidsDokumen11 halamanAccessory Structures of The Eye: (Photoreceptors) Sense and EyelidsJieun BaekBelum ada peringkat
- Axial Bones OutlineDokumen78 halamanAxial Bones Outlineseribongie is stu dyingBelum ada peringkat
- Ear HistologyDokumen3 halamanEar HistologyGrace Shan Bernus100% (1)
- Hip Bone, Medial ViewDokumen1 halamanHip Bone, Medial ViewRitik SinghBelum ada peringkat
- Neuroscience Pre-Midterm Pathways: Fall 2012Dokumen46 halamanNeuroscience Pre-Midterm Pathways: Fall 2012Yezin ShamoonBelum ada peringkat
- RespiratoryanatomyDokumen5 halamanRespiratoryanatomyMary♡Belum ada peringkat
- Posterio Approach Subaxial Cervical Spine + Anterior Approach Cervical Spine +aplied Surgical AnatomyDokumen28 halamanPosterio Approach Subaxial Cervical Spine + Anterior Approach Cervical Spine +aplied Surgical AnatomywidapnBelum ada peringkat
- Stem12bsn2 Casestudy5 PDFDokumen12 halamanStem12bsn2 Casestudy5 PDFShane TabalbaBelum ada peringkat
- Red EyeDokumen49 halamanRed EyeJonathan Cua Lim100% (1)
- Blepharitis - UpToDateDokumen22 halamanBlepharitis - UpToDateanisa maria ulfaBelum ada peringkat
- Med Surg Sensory Sample PDFDokumen30 halamanMed Surg Sensory Sample PDFShucipto DwiBelum ada peringkat
- Ophthalmology Osce Exam - PPTX PP by Abel - 230170110143Dokumen86 halamanOphthalmology Osce Exam - PPTX PP by Abel - 230170110143Chefera Aga100% (1)
- Ophthalmology Review Manual 2nd EditionDokumen538 halamanOphthalmology Review Manual 2nd EditionAnonymous 4OnqyBErBelum ada peringkat
- Dr. Mubashir Rehman: Assistant ProfessorDokumen112 halamanDr. Mubashir Rehman: Assistant Professorsaqibullah gulBelum ada peringkat
- Clinical Skills of Eye Examination: by Dr. Hajer Ahmed Ophthalmology Specialist Omar Almukhtar University 2019-2020Dokumen40 halamanClinical Skills of Eye Examination: by Dr. Hajer Ahmed Ophthalmology Specialist Omar Almukhtar University 2019-2020Helene AlawamiBelum ada peringkat
- Dry Eye Syndrome OverviewDokumen7 halamanDry Eye Syndrome OverviewhaninamaulianiBelum ada peringkat
- Journal Reading - HordeolumDokumen20 halamanJournal Reading - HordeolumsnylstlBelum ada peringkat
- Blepharitis - Medical Disability GuidelinesDokumen3 halamanBlepharitis - Medical Disability GuidelinesFerni ArmantiBelum ada peringkat
- Microbiology For OptometristsDokumen7 halamanMicrobiology For OptometristsMohamed Shantier100% (2)
- Emergency Eye Care WorkshopDokumen21 halamanEmergency Eye Care WorkshopAriani Ratri Dewi100% (1)
- Blepharitis (Inflammation of The Lid Margins) : Demodex Brevis Mite Infestation)Dokumen4 halamanBlepharitis (Inflammation of The Lid Margins) : Demodex Brevis Mite Infestation)Chad McleanBelum ada peringkat
- SYNNAA OphthalmologyDokumen56 halamanSYNNAA OphthalmologyAbdul RehmanBelum ada peringkat
- A&E BlepharitisDokumen3 halamanA&E BlepharitisNadine Bär-SchmitzBelum ada peringkat
- Ophthalmology MCQsDokumen173 halamanOphthalmology MCQsvamshidh33% (3)
- MCQs Faeza Fcps Opth Past PapersDokumen136 halamanMCQs Faeza Fcps Opth Past Papershasan aslamBelum ada peringkat
- Prevalence of Eyelid Diseases Among Adults in Hong Kong: Shiu Ting Mak, Sze Wai Jeremy John Kwok, Hunter KL YuenDokumen4 halamanPrevalence of Eyelid Diseases Among Adults in Hong Kong: Shiu Ting Mak, Sze Wai Jeremy John Kwok, Hunter KL YuenAndrewBelum ada peringkat
- MCQ Kamal 2021Dokumen26 halamanMCQ Kamal 2021king darkBelum ada peringkat
- #The EyelidDokumen7 halaman#The Eyelidameerabest100% (1)
- Eye Lids: Anatomy of Eye LidDokumen14 halamanEye Lids: Anatomy of Eye Lidhenry caze100% (1)
- Chalazion Risk Factors: A Review Article: Ophthalmology Department, Ohud Hospital, Madina, Saudi ArabiaDokumen6 halamanChalazion Risk Factors: A Review Article: Ophthalmology Department, Ohud Hospital, Madina, Saudi ArabiaLIZBETH MORALES VALDIVIABelum ada peringkat
- Notes - Notes - Ophthalmology PDFDokumen30 halamanNotes - Notes - Ophthalmology PDFRumana Ali100% (2)
- Eye Essentials Rigid Gas Permeable Lens FittingDokumen198 halamanEye Essentials Rigid Gas Permeable Lens FittingUsman ImtiazBelum ada peringkat
- Eyelid Disorders: Ii. ChalazionDokumen62 halamanEyelid Disorders: Ii. ChalazionFreeburn SimunchembuBelum ada peringkat
- Jop 2017 0052 PDFDokumen15 halamanJop 2017 0052 PDFAbdul Jalil MondalBelum ada peringkat
- Red EyeDokumen6 halamanRed EyeafatBelum ada peringkat
- 1 PBDokumen4 halaman1 PBRian YupitaBelum ada peringkat
- Case Study BlepharitisDokumen12 halamanCase Study BlepharitisNorshahidah IedaBelum ada peringkat