Anda mungkin juga menyukai
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- A Critical Overview of Abortion in IndiaDokumen15 halamanA Critical Overview of Abortion in IndiaAnta SharmaBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Individual Activity #3: CHAPTER STUDY QUESTIONS: Rubric For Short AnswerDokumen11 halamanIndividual Activity #3: CHAPTER STUDY QUESTIONS: Rubric For Short AnswerSatanichia McDowell KurumizawaBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- ComplicationsDokumen22 halamanComplicationsLyra LoonBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Breastfeeding Uncovering Barriers and Offering SolutionsDokumen6 halamanBreastfeeding Uncovering Barriers and Offering SolutionsSuéllen EmidioBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Dirty DictionaryDokumen124 halamanDirty DictionarySEX52% (23)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- GonadoDokumen32 halamanGonadoshailendra meena50% (2)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- InfertilityDokumen29 halamanInfertilityCristina StanleeBelum ada peringkat
- Sande's HIV - AIDS Medicine (PDFDrive)Dokumen562 halamanSande's HIV - AIDS Medicine (PDFDrive)angel muñozBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Lapjag Poli Obgyn 27-29 April 2021 (KLMPK Syifa)Dokumen13 halamanLapjag Poli Obgyn 27-29 April 2021 (KLMPK Syifa)Adi Joyo NegoroBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Changes in AdolescenceDokumen32 halamanChanges in AdolescenceLei Anne Vieve Lumbog100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Ovarian Cycle.Dokumen20 halamanThe Ovarian Cycle.Salman KhanBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Recording and Reporting Based On FHSISDokumen40 halamanRecording and Reporting Based On FHSISAnonymous h2EnKyDbBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Bringing The Illusion To Light Legalization of ProstitutionDokumen2 halamanBringing The Illusion To Light Legalization of ProstitutionleiaoblenaBelum ada peringkat
- Relationships: Latin Key WordsDokumen2 halamanRelationships: Latin Key WordsIanua ViteBelum ada peringkat
- PreeclampsiaDokumen27 halamanPreeclampsiairon100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Fisiologi PersalinanDokumen29 halamanFisiologi PersalinanichaBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- ChildMarriage Malaysia WorkingPaper v2Dokumen93 halamanChildMarriage Malaysia WorkingPaper v2syuBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Gestational Trophoblastic Diseases Hydatiform MoleDokumen40 halamanGestational Trophoblastic Diseases Hydatiform MoleL3SBelum ada peringkat
- Jurnal Dr. SoebandiDokumen7 halamanJurnal Dr. SoebandiRia atistianiBelum ada peringkat
- ThesisDokumen11 halamanThesispriyankaBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
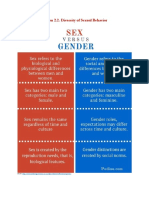
- Sexuality and Gender PDFDokumen4 halamanSexuality and Gender PDFNeil Vincent BocoBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Annex A. Monthly Reporting Matrix (MRM) - Streamlined VersionDokumen4 halamanAnnex A. Monthly Reporting Matrix (MRM) - Streamlined VersionPatricio Perez CabahugBelum ada peringkat
- What Is SyphilisDokumen12 halamanWhat Is SyphilisBheru LalBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Cord Presentation and ProlapseDokumen7 halamanCord Presentation and ProlapseIsrael WoseneBelum ada peringkat
- Female Genital MutilationDokumen17 halamanFemale Genital MutilationDanty DanestriaBelum ada peringkat
- MDWF 2020 Carter 6Dokumen13 halamanMDWF 2020 Carter 6api-366292665Belum ada peringkat
- Davis 2020Dokumen7 halamanDavis 2020Erdiwan MandanBelum ada peringkat
- Non Penetrative SexDokumen8 halamanNon Penetrative SexnathanBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Laws On ChildrenDokumen143 halamanLaws On ChildrenJoel SerranoBelum ada peringkat
- NSVDDokumen48 halamanNSVDchiqui14100% (2)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)