Anda mungkin juga menyukai
- Management and Medications in Thyroid Strom and Myxoedema ComaDokumen41 halamanManagement and Medications in Thyroid Strom and Myxoedema ComaBhavesh kunvarBelum ada peringkat
- Thyroid & Anti-Thyroid DrugsDokumen59 halamanThyroid & Anti-Thyroid DrugsNiranjanBelum ada peringkat
- 11 - Drugs For Thyroid Problems2Dokumen51 halaman11 - Drugs For Thyroid Problems2nica velanoBelum ada peringkat
- Thyroid DrugsDokumen6 halamanThyroid DrugsThe Real UploaderBelum ada peringkat
- Thyroid DisordersDokumen34 halamanThyroid DisordersAbdulhameed Mohamed100% (1)
- Anti-Thyroid Drugs and Thyroid HormoneDokumen7 halamanAnti-Thyroid Drugs and Thyroid Hormonemicheal1960100% (1)
- Thyroid Disorders - 2023Dokumen82 halamanThyroid Disorders - 2023JEPHTHAH KWASI DANSOBelum ada peringkat
- 14) Drugs For Thyroid DisordersDokumen13 halaman14) Drugs For Thyroid DisordersLatiBelum ada peringkat
- Endocrinology Board Review: Thyroid DisordersDokumen46 halamanEndocrinology Board Review: Thyroid DisordersDemuel Dee L. BertoBelum ada peringkat
- CombinedDokumen40 halamanCombinedshortsmotivation87Belum ada peringkat
- Endocrine Pharmacology: Thyroid & AntithyroidDokumen54 halamanEndocrine Pharmacology: Thyroid & AntithyroidRegina CiputraBelum ada peringkat
- The Thyroid Gland PRINT 2021Dokumen9 halamanThe Thyroid Gland PRINT 2021abcde990075Belum ada peringkat
- Thyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoDokumen35 halamanThyrotoxicosis: Presenter: Emiacu Kenneth Facilitator: Dr. Freddie KibengoNinaBelum ada peringkat
- Anti - Thyroid Drugs: Renju.S.RaviDokumen27 halamanAnti - Thyroid Drugs: Renju.S.RavidrfatimarizBelum ada peringkat
- Lesson 6 Thyroid and Antithyroid DrugsDokumen28 halamanLesson 6 Thyroid and Antithyroid DrugstheintrovBelum ada peringkat
- Thyroid CrisisDokumen34 halamanThyroid CrisisRidyah Ning TyasBelum ada peringkat
- Thyroid & Antithyroid Drugs - 2020Dokumen7 halamanThyroid & Antithyroid Drugs - 2020ireneBelum ada peringkat
- W3-14 Thyroid and Parathyroid Hormones LectureDokumen33 halamanW3-14 Thyroid and Parathyroid Hormones LectureVivekBelum ada peringkat
- Thyroid Gland and Diseases of Thyroid Gland: DR - Ranadhi Das MD - PGT, Dept of PhysiologyDokumen75 halamanThyroid Gland and Diseases of Thyroid Gland: DR - Ranadhi Das MD - PGT, Dept of Physiologysam mehraBelum ada peringkat
- Hyperthyroidsm: EpidemiologyDokumen6 halamanHyperthyroidsm: EpidemiologyEllieBelum ada peringkat
- Thyroid Hormones & DrugsDokumen51 halamanThyroid Hormones & DrugsSUTHANBelum ada peringkat
- 27 - CC SAN ANTONIO - Hypothyroidism, Hyper, Thyroid Nodular Disease and CancerDokumen77 halaman27 - CC SAN ANTONIO - Hypothyroidism, Hyper, Thyroid Nodular Disease and CancerDann San AntonioBelum ada peringkat
- Thyrotoxicosis & Hypothyroidism by Prof DR NK ChopraDokumen52 halamanThyrotoxicosis & Hypothyroidism by Prof DR NK ChopraAbdulsalam DostBelum ada peringkat
- Pharmacology of ThyroidDokumen32 halamanPharmacology of Thyroidbrigita charvioBelum ada peringkat
- Thyroid and Antithyroid Agent-VDokumen60 halamanThyroid and Antithyroid Agent-VVine100% (1)
- Theme 2: Thyroid Diseases: Study GoalsDokumen9 halamanTheme 2: Thyroid Diseases: Study GoalsOlesyaBelum ada peringkat
- HipotiroidDokumen28 halamanHipotiroidmeongkorengBelum ada peringkat
- FKG3 - Pharmacology of Thyroid GlandsDokumen28 halamanFKG3 - Pharmacology of Thyroid GlandsRhena Fitria KhairunnisaBelum ada peringkat
- 2 TSHDokumen7 halaman2 TSHNashat SaadiBelum ada peringkat
- Anti Thyroid DrugsDokumen38 halamanAnti Thyroid Drugsone_nd_onlyuBelum ada peringkat
- Anti-Thyroid DrugsDokumen17 halamanAnti-Thyroid DrugsVersatile UnitBelum ada peringkat
- Hypothyroid in Pregnancy Andi CakraDokumen32 halamanHypothyroid in Pregnancy Andi CakraCakraEkkyBelum ada peringkat
- HipotiroidDokumen28 halamanHipotiroidReza SatriaBelum ada peringkat
- Thyroid and Parathyroid GlandsDokumen133 halamanThyroid and Parathyroid GlandsmunafalmahdiBelum ada peringkat
- 3ES-2 Thyroid and Antithyroid Drugs 1436Dokumen46 halaman3ES-2 Thyroid and Antithyroid Drugs 1436Muath AlqarniBelum ada peringkat
- Thyroid & Antithyroid DrugsDokumen27 halamanThyroid & Antithyroid DrugsjabirBelum ada peringkat
- Pharmacology of Thyroid HormonesDokumen56 halamanPharmacology of Thyroid HormonesDr.U.P.Rathnakar.MD.DIH.PGDHMBelum ada peringkat
- Endocrine Pharmacology by DR - Mayur SaytaDokumen27 halamanEndocrine Pharmacology by DR - Mayur Saytasahilthakker2012Belum ada peringkat
- 3 Use Thyroid Gland Use TTDokumen55 halaman3 Use Thyroid Gland Use TTMathy MtenjeBelum ada peringkat
- DR Ananta Thyroid SlideDokumen73 halamanDR Ananta Thyroid SlideRoshan Kumar PanditBelum ada peringkat
- HSP2 Topic 4 Part 3 (Thyroid Disorders)Dokumen56 halamanHSP2 Topic 4 Part 3 (Thyroid Disorders)gilliansong17Belum ada peringkat
- Hypothyroidism 2Dokumen50 halamanHypothyroidism 2Ziaur rabbi sakilBelum ada peringkat
- Anti-Thyroid and Thyroid DrugsDokumen36 halamanAnti-Thyroid and Thyroid DrugsDylan MansillaBelum ada peringkat
- 2 Thyroid and Antithyroid DrugsDokumen24 halaman2 Thyroid and Antithyroid DrugsLiza Marie de Guzman100% (1)
- HormonesDokumen64 halamanHormonesNiyaz ShahriarBelum ada peringkat
- Intro To The Function of Thyroid GlandDokumen35 halamanIntro To The Function of Thyroid Glandinka.elseBelum ada peringkat
- HipothyroidDokumen48 halamanHipothyroidCakraEkkyBelum ada peringkat
- Trachea: Thyroid Agents Thyroid Gland Is Located in The Middle of The Neck and SurroundsDokumen10 halamanTrachea: Thyroid Agents Thyroid Gland Is Located in The Middle of The Neck and SurroundsMIR SARTAJBelum ada peringkat
- CC 3-Lab FKM 17Dokumen4 halamanCC 3-Lab FKM 17mayabangkurtipotBelum ada peringkat
- Hepatotoxicity, Vasculitis:: Pruritic Rash, Arthralgias-Joint Pain, AgranulocytosisDokumen3 halamanHepatotoxicity, Vasculitis:: Pruritic Rash, Arthralgias-Joint Pain, AgranulocytosisThuan Tăng NguyenBelum ada peringkat
- Dr. Nesrine Salah El Dine: Thyroid Gland From Pharmacology To Clinical PracticeDokumen24 halamanDr. Nesrine Salah El Dine: Thyroid Gland From Pharmacology To Clinical Practiceamaal ramadanBelum ada peringkat
- BP503T Unit 4-6Dokumen60 halamanBP503T Unit 4-6Solomon GyampohBelum ada peringkat
- Bp503t Pcol Unit-IVDokumen14 halamanBp503t Pcol Unit-IVBaraa AbdalrazaqBelum ada peringkat
- 05 Chapter Endrocrine SystemDokumen40 halaman05 Chapter Endrocrine SystemMSKCBelum ada peringkat
- Drugs Acting in The Endocrine SystemDokumen19 halamanDrugs Acting in The Endocrine SystemPrincess C. SultanBelum ada peringkat
- Thyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsDokumen7 halamanThyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsPrincess Noreen SavellanoBelum ada peringkat
- THYROIDDokumen17 halamanTHYROIDvinolashrimmishma.sBelum ada peringkat
- Thyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!Dari EverandThyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!Belum ada peringkat
- Hyperthyroidism, A Simple Guide To The Condition, Treatment And Related ConditionsDari EverandHyperthyroidism, A Simple Guide To The Condition, Treatment And Related ConditionsPenilaian: 2 dari 5 bintang2/5 (2)
- Goodpasture's Syndrome, Hashimoto's Thyroiditis, Graves's Disease & Type I DiabetesDokumen2 halamanGoodpasture's Syndrome, Hashimoto's Thyroiditis, Graves's Disease & Type I DiabetesZara MohammedBelum ada peringkat
- Papillary Thyroid CarcinomaDokumen17 halamanPapillary Thyroid CarcinomaEster Sibarani100% (2)
- Solitary Nodule of Thyroid Gland: An Overview and Case StudyDokumen3 halamanSolitary Nodule of Thyroid Gland: An Overview and Case StudyInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Thyroid by Dr. Shyam Kalavalapalli, Endocrinologist, HyderabadDokumen87 halamanThyroid by Dr. Shyam Kalavalapalli, Endocrinologist, HyderabadSherman BellBelum ada peringkat
- The Following Are A Selection of Clinical Biochemistry Part 1 Exam Questions Retired From The College Question Bank in December 2020Dokumen14 halamanThe Following Are A Selection of Clinical Biochemistry Part 1 Exam Questions Retired From The College Question Bank in December 2020كن مع الله100% (1)
- MCQ Question SheetDokumen6 halamanMCQ Question SheethappyhappylandBelum ada peringkat
- Sujok Therapy and Treatment of Diseases Part IiDokumen7 halamanSujok Therapy and Treatment of Diseases Part IiDoctor A SethiBelum ada peringkat
- Ultrasound NotesDokumen19 halamanUltrasound NotesJihad Anad100% (1)
- Endo MCQs Backup 2020Dokumen213 halamanEndo MCQs Backup 2020Giridhar SolasaBelum ada peringkat
- Common Medical AbbreviationDokumen25 halamanCommon Medical AbbreviationKim Glaidyl BontuyanBelum ada peringkat
- Recent EMF PapersDokumen1.068 halamanRecent EMF PapersSaliendo del HipercuboBelum ada peringkat
- How To Interpret Thyroid Function TestsDokumen5 halamanHow To Interpret Thyroid Function TestsnonieshzBelum ada peringkat
- Hormones: Prof. Dr. V P SoniDokumen21 halamanHormones: Prof. Dr. V P SoniPadma VishwanathBelum ada peringkat
- NeurotransmittersDokumen4 halamanNeurotransmittersSalman Khan100% (1)
- Unit 3 Endocrine SystemDokumen36 halamanUnit 3 Endocrine SystemdhanashriBelum ada peringkat
- Health Assessment 10Dokumen11 halamanHealth Assessment 10shannon c. lewisBelum ada peringkat
- Chemical Coordination 1Dokumen22 halamanChemical Coordination 1SureshBelum ada peringkat
- ReportDokumen3 halamanReportFascino WhiteBelum ada peringkat
- © Ncert Not To Be Republished: C C I C 22Dokumen17 halaman© Ncert Not To Be Republished: C C I C 22SatyarthShuklaBelum ada peringkat
- Thyroid QuizDokumen3 halamanThyroid QuizĐặng Quỳnh ANBelum ada peringkat
- Diffuse Toxic GoiterDokumen64 halamanDiffuse Toxic GoiterMuftihat IsrarBelum ada peringkat
- SketchyPath ChecklistDokumen1 halamanSketchyPath ChecklistGabriella RosinaBelum ada peringkat
- Department of Hormones: 25 - Hydroxy Vitamin DDokumen2 halamanDepartment of Hormones: 25 - Hydroxy Vitamin DKrishnaveni . BBelum ada peringkat
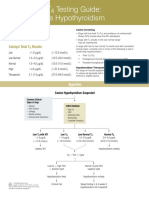
- Catalyst One Total t4 Testing Guide en PDFDokumen2 halamanCatalyst One Total t4 Testing Guide en PDFИрина ВладимироваBelum ada peringkat
- Z045 PDFDokumen2 halamanZ045 PDFAayushi SadaniBelum ada peringkat
- Sub Q ManualDokumen27 halamanSub Q ManualArturo Loredo100% (1)
- The Endocrine System NotesDokumen11 halamanThe Endocrine System NotesArce JohnsonBelum ada peringkat
- Case Study (Goiter)Dokumen41 halamanCase Study (Goiter)yasira100% (1)
- 17-Ebcpg Thyroid2013Dokumen20 halaman17-Ebcpg Thyroid2013Mi MingkaiBelum ada peringkat
- Rietz Thyroid Final PDFDokumen50 halamanRietz Thyroid Final PDFRoberto CortezBelum ada peringkat