Anda mungkin juga menyukai
- 13 Profesionalism and Managerial SkillDokumen16 halaman13 Profesionalism and Managerial SkillTiaRa JuraidBelum ada peringkat
- Xenobiotics 2015Dokumen52 halamanXenobiotics 2015TiaRa JuraidBelum ada peringkat
- 11 Kesehatan MasyarakatDokumen48 halaman11 Kesehatan MasyarakatTiaRa JuraidBelum ada peringkat
- Ormood Aits ,: Tory Failure Reaso, As For Which May Be The Primary ReasonDokumen6 halamanOrmood Aits ,: Tory Failure Reaso, As For Which May Be The Primary ReasonTiaRa JuraidBelum ada peringkat
- Translate Part 1Dokumen22 halamanTranslate Part 1TiaRa JuraidBelum ada peringkat
- 16 English in MedicineDokumen15 halaman16 English in MedicineTiaRa JuraidBelum ada peringkat
- Department of Histology and Cell Biology Faculty of Medicine Universitas Gadjah MadaDokumen14 halamanDepartment of Histology and Cell Biology Faculty of Medicine Universitas Gadjah MadaTiaRa JuraidBelum ada peringkat
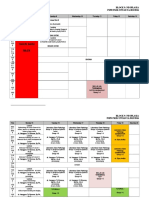
- Block 10: Musculoskeletal and Locomotion PSPD FKIK UNTAD TA. 2015/2016 WEEK 1: 28 Maret - 2 April 2016Dokumen7 halamanBlock 10: Musculoskeletal and Locomotion PSPD FKIK UNTAD TA. 2015/2016 WEEK 1: 28 Maret - 2 April 2016TiaRa JuraidBelum ada peringkat
- Jadwal Blok 9 Untad 2016 Rev 25012016Dokumen7 halamanJadwal Blok 9 Untad 2016 Rev 25012016TiaRa JuraidBelum ada peringkat
- Metabolic Rate Dan BMR: DR - Dr.zaenal M. Sofro, AIFM, Sport & Circ. Med. Bagian Ilmu Faal Fak - Kedokteran UGMDokumen78 halamanMetabolic Rate Dan BMR: DR - Dr.zaenal M. Sofro, AIFM, Sport & Circ. Med. Bagian Ilmu Faal Fak - Kedokteran UGMTiaRa JuraidBelum ada peringkat
- Musculoskeletal SystemDokumen76 halamanMusculoskeletal SystemTiaRa JuraidBelum ada peringkat
- LO Blok 22 Skenario 3Dokumen5 halamanLO Blok 22 Skenario 3TiaRa JuraidBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Summative Reflection FinalDokumen8 halamanSummative Reflection Finalapi-432057546Belum ada peringkat
- Whitefish CareDokumen32 halamanWhitefish CareNBC MontanaBelum ada peringkat
- Philippine Health Care Providers Vs CIR (MR)Dokumen2 halamanPhilippine Health Care Providers Vs CIR (MR)Jonathan DancelBelum ada peringkat
- Hospital PricingDokumen41 halamanHospital Pricingaarti HingeBelum ada peringkat
- Palm Pistol - What People Are SayingDokumen17 halamanPalm Pistol - What People Are SayingAmmoLand Shooting Sports NewsBelum ada peringkat
- Sulfa Nil Amide Deaths of 1937Dokumen4 halamanSulfa Nil Amide Deaths of 1937api-3810976Belum ada peringkat
- AHMMoclDokumen140 halamanAHMMoclvandyranaBelum ada peringkat
- Mean Street Minsitry Resource Guide by Appointment Only: Mailing AddressDokumen44 halamanMean Street Minsitry Resource Guide by Appointment Only: Mailing AddressFrankie BlankenshipBelum ada peringkat
- Sample Part A Medicare Summary NoticeDokumen6 halamanSample Part A Medicare Summary NoticejerilBelum ada peringkat
- Health Care Case-1Dokumen8 halamanHealth Care Case-1Krishnamohan VaddadiBelum ada peringkat
- U.S. Healthcare in Need of SurgeryDokumen7 halamanU.S. Healthcare in Need of SurgerytonyonetonBelum ada peringkat
- The Impact of Technology in Clinical TechnologyDokumen3 halamanThe Impact of Technology in Clinical TechnologyMiki NishiharaBelum ada peringkat
- Defining Patient Safety and Quality CareDokumen6 halamanDefining Patient Safety and Quality CareswethashakiBelum ada peringkat
- Call Center Staff CompetenciesDokumen2 halamanCall Center Staff CompetenciesCarianne JohnsonBelum ada peringkat
- Living WillDokumen2 halamanLiving Willapi-317496261Belum ada peringkat
- Phone Call TranscriptDokumen11 halamanPhone Call TranscriptKevinSeanHeldBelum ada peringkat
- Little Sisters of The PoorDokumen10 halamanLittle Sisters of The Poorapi-253390668Belum ada peringkat
- Akorn DetailDokumen16 halamanAkorn DetailavtarsinghsadafBelum ada peringkat
- UNICARE Company ProfileDokumen7 halamanUNICARE Company ProfileMarjorie UnicareBelum ada peringkat
- Hospital Performance IndicatorsDokumen2 halamanHospital Performance IndicatorsAyunda Raisha IsmandiyaBelum ada peringkat
- Billing Guidance For Pharmacists Professional and Patient Care Services White PaperDokumen9 halamanBilling Guidance For Pharmacists Professional and Patient Care Services White Paperkrishna krBelum ada peringkat
- Valproate SOP PDFDokumen11 halamanValproate SOP PDFIwan IrawanBelum ada peringkat
- Demographics of The Aging PeopleDokumen12 halamanDemographics of The Aging Peoplealfandhi100% (1)
- Volkswagen India Embarks On A New CSR Project Starts Operating Mobile Health Clinic in Khed TalukaDokumen3 halamanVolkswagen India Embarks On A New CSR Project Starts Operating Mobile Health Clinic in Khed TalukaVWPunePlantBelum ada peringkat
- Telemedicine/Telehealth in The PhilippinesDokumen3 halamanTelemedicine/Telehealth in The PhilippinesangelBelum ada peringkat
- Bed Rail Brochure - DSHSDokumen2 halamanBed Rail Brochure - DSHSIsaiah FedurBelum ada peringkat
- Vision RehabilitationDokumen46 halamanVision RehabilitationDrGENBelum ada peringkat
- Email To Monique Mccollum 1 13 14Dokumen7 halamanEmail To Monique Mccollum 1 13 14api-244230664Belum ada peringkat
- Region 7 HospitalDokumen8 halamanRegion 7 HospitalBart TareBelum ada peringkat
- PMK Manifesto - Tamilnadu Election 2016Dokumen96 halamanPMK Manifesto - Tamilnadu Election 2016karkotaganBelum ada peringkat