Anda mungkin juga menyukai
- Abortion PresentationDokumen46 halamanAbortion PresentationJhong Xyrus67% (3)
- Pelvic Organ Prolapse GuideDokumen48 halamanPelvic Organ Prolapse GuideKerod AbebeBelum ada peringkat
- Uterine FibroidsDokumen21 halamanUterine FibroidsPrasun BiswasBelum ada peringkat
- Obstetric Anal Sphincter Injury (OASIS) - UpToDateDokumen39 halamanObstetric Anal Sphincter Injury (OASIS) - UpToDateErickBelum ada peringkat
- Evaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusDokumen7 halamanEvaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusGabyliz Gonzalez CastilloBelum ada peringkat
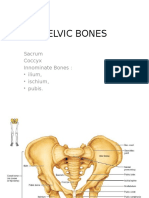
- Pelvic BoneDokumen15 halamanPelvic BoneYoanneveline TanakBelum ada peringkat
- Mullarian AnomoliesDokumen85 halamanMullarian AnomoliesPrathibha GuruguriBelum ada peringkat
- Genital FistulaeDokumen15 halamanGenital Fistulaesangeetha francisBelum ada peringkat
- Pop QDokumen45 halamanPop QObgyn Maret2016Belum ada peringkat
- Spontaneous Delivery in Post-Term PregnancyDokumen55 halamanSpontaneous Delivery in Post-Term Pregnancyr.pavinvikneshBelum ada peringkat
- Malig Ovarian TumoursDokumen42 halamanMalig Ovarian TumoursSamuel InbarajaBelum ada peringkat
- Difficulties in Vaginal HysterctomyDokumen66 halamanDifficulties in Vaginal HysterctomyManamita NiphadkarBelum ada peringkat
- Myop in PregnancyDokumen4 halamanMyop in PregnancySamuel WilliamsBelum ada peringkat
- Acog Practice Bulletin Summary: Pregestational Diabetes MellitusDokumen3 halamanAcog Practice Bulletin Summary: Pregestational Diabetes MellitusMaría Fernanda Palma AcostaBelum ada peringkat
- Lower and Upper Genital Tract InfectionsDokumen170 halamanLower and Upper Genital Tract InfectionsDanna BongonBelum ada peringkat
- Cardiac Disease in PregnancyDokumen28 halamanCardiac Disease in PregnancyviharadewiBelum ada peringkat
- Preterm Labour: Management GuidelinesDokumen44 halamanPreterm Labour: Management Guidelinesvacha sardarBelum ada peringkat
- Kuliah GastroDokumen119 halamanKuliah GastroMonazzt AsshagabBelum ada peringkat
- Ventric Ul Omega LyDokumen40 halamanVentric Ul Omega LyErliana FaniBelum ada peringkat
- Recurrent UTI Case Presentation in Child with Obstructive UropathyDokumen26 halamanRecurrent UTI Case Presentation in Child with Obstructive UropathyAminath MeesanBelum ada peringkat
- Infertility IDokumen36 halamanInfertility Idr_asaleh100% (1)
- ALARMER Dystocia PDFDokumen5 halamanALARMER Dystocia PDFwilliamBelum ada peringkat
- Pathology of The AdnexaDokumen59 halamanPathology of The AdnexaArnella HutagalungBelum ada peringkat
- Pregnancy and Labor at Fetal Malpresentations and Abnormal PelvisDokumen40 halamanPregnancy and Labor at Fetal Malpresentations and Abnormal PelvisCoral Srinivasa Ramalu100% (1)
- Carcinoma Rectum - Janak - NEWDokumen74 halamanCarcinoma Rectum - Janak - NEWTowhidulIslamBelum ada peringkat
- Acute Abdominal Pain in Pregnancy: Diagnosis and Management Conservative vs. SurgicalDokumen73 halamanAcute Abdominal Pain in Pregnancy: Diagnosis and Management Conservative vs. SurgicalIgnatov OanaBelum ada peringkat
- Laparoscopic Gynecologist Surgeon in HSR Layout BangaloreDokumen8 halamanLaparoscopic Gynecologist Surgeon in HSR Layout BangaloreDr.Beena JeysinghBelum ada peringkat
- Vaginal Vault ProlapseDokumen9 halamanVaginal Vault ProlapseOanaBelum ada peringkat
- Missed AbortionDokumen45 halamanMissed AbortionMarest AskynaBelum ada peringkat
- Benign Neoplasm of OvaryDokumen60 halamanBenign Neoplasm of OvaryMimie SabrinaBelum ada peringkat
- Ovarian Torsion PDFDokumen35 halamanOvarian Torsion PDFitshijabi vlogsBelum ada peringkat
- Molar PregnancyDokumen14 halamanMolar Pregnancyfardeal_mckk100% (1)
- Ca VulvaDokumen38 halamanCa VulvavincentsharonBelum ada peringkat
- First Trimester BleedingDokumen12 halamanFirst Trimester BleedingKevin de SilvaBelum ada peringkat
- Management of Monochorionic Twin Pregnancy: Green-Top Guideline No. 51Dokumen13 halamanManagement of Monochorionic Twin Pregnancy: Green-Top Guideline No. 51indra_strongBelum ada peringkat
- Fetal Healt Survillence SCOGDokumen55 halamanFetal Healt Survillence SCOGCésar Gardeazábal100% (1)
- Obstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006Dokumen559 halamanObstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006fagiy51113Belum ada peringkat
- Amnioinfusion Guide: Functions, Indications, Procedures"TITLE"All about Amnioinfusion - What it is, When Used, Process" TITLE"Complete Amnioinfusion Overview - Definition, Benefits, RisksDokumen16 halamanAmnioinfusion Guide: Functions, Indications, Procedures"TITLE"All about Amnioinfusion - What it is, When Used, Process" TITLE"Complete Amnioinfusion Overview - Definition, Benefits, RiskstapayanaBelum ada peringkat
- Impey Obs and Gynae Revision Notes PDFDokumen9 halamanImpey Obs and Gynae Revision Notes PDFRoiseBelum ada peringkat
- Evidence-Based Management of Endometrioma: Tarek A Gelbaya, Luciano G NardoDokumen10 halamanEvidence-Based Management of Endometrioma: Tarek A Gelbaya, Luciano G NardofebrianoramadhanaBelum ada peringkat
- Pelvic Inflammatory Disease by SlidesgoDokumen51 halamanPelvic Inflammatory Disease by SlidesgoGina MorenoBelum ada peringkat
- 2015 Oncology CREOG Review PDFDokumen76 halaman2015 Oncology CREOG Review PDFRima HajjarBelum ada peringkat
- Pterigium: Dr. Purnamanita Syawal, SPM, MarsDokumen39 halamanPterigium: Dr. Purnamanita Syawal, SPM, Marsyayat muhammadBelum ada peringkat
- Testicular TorsionDokumen12 halamanTesticular TorsionlicutBelum ada peringkat
- Ovarian Cyst Types and SymptomsDokumen17 halamanOvarian Cyst Types and SymptomsLim Su-WeiBelum ada peringkat
- Obs History Taking FormatDokumen24 halamanObs History Taking FormatBibek PandeyBelum ada peringkat
- Judi Januadi Endjun: Gatot Soebroto Army Central Hospital/ Medical Faculty, University of Indonesia ISUOG, Bali, 2009Dokumen66 halamanJudi Januadi Endjun: Gatot Soebroto Army Central Hospital/ Medical Faculty, University of Indonesia ISUOG, Bali, 2009Judi Januadi Endjun, MD, ObsGynBelum ada peringkat
- CERVICAL LYMPADENOPATHY - EduardDokumen34 halamanCERVICAL LYMPADENOPATHY - EduardYemima Divinadia100% (1)
- Table 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationDokumen111 halamanTable 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationArya Syafaromania RachmaBelum ada peringkat
- Kehamilan MolaDokumen88 halamanKehamilan MolaYhanna UlfianiBelum ada peringkat
- Cme Fast ScanDokumen25 halamanCme Fast Scannirmal raj100% (1)
- Urinary Tract Infections Pregnancy PDFDokumen19 halamanUrinary Tract Infections Pregnancy PDFNay Lin HtikeBelum ada peringkat
- ULTRASOUND Fetal AnomaliesdocxDokumen86 halamanULTRASOUND Fetal AnomaliesdocxAlexandra MateiBelum ada peringkat
- 62 Colposcopy StandardsDokumen73 halaman62 Colposcopy Standardsrijal mahdiy pBelum ada peringkat
- MENSTRUAL DISORDERS: CAUSES, DIAGNOSIS AND MANAGEMENTDokumen36 halamanMENSTRUAL DISORDERS: CAUSES, DIAGNOSIS AND MANAGEMENTAkinbani MoyosoreBelum ada peringkat
- Abortion and Sterilization: Medical and Social AspectsDari EverandAbortion and Sterilization: Medical and Social AspectsJane E. HodgsonBelum ada peringkat
- Handbook of Current and Novel Protocols for the Treatment of InfertilityDari EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanBelum ada peringkat
- 2023 OB/GYN Coding Manual: Components of Correct CodingDari Everand2023 OB/GYN Coding Manual: Components of Correct CodingBelum ada peringkat
- Hypospadias Surgery: An Illustrated GuideDari EverandHypospadias Surgery: An Illustrated GuideAhmed HadidiPenilaian: 5 dari 5 bintang5/5 (1)
- Occupational Health and Safety (OHS) Issues in by G S BerihaDokumen201 halamanOccupational Health and Safety (OHS) Issues in by G S Berihatanmai nooluBelum ada peringkat
- Unit 3Dokumen46 halamanUnit 3tanmai nooluBelum ada peringkat
- Disaster Nursing SeminarDokumen41 halamanDisaster Nursing Seminartanmai nooluBelum ada peringkat
- Standards and ProtocolsDokumen16 halamanStandards and Protocolstanmai nooluBelum ada peringkat
- PsychologyDokumen5 halamanPsychologytanmai nooluBelum ada peringkat
- Faculity of Nursing Chapter - Viii SociologyDokumen49 halamanFaculity of Nursing Chapter - Viii Sociologytanmai nooluBelum ada peringkat
- Clinical TeachingDokumen21 halamanClinical Teachingtanmai nooluBelum ada peringkat
- G&D Assessment Infant SpacingDokumen2 halamanG&D Assessment Infant Spacingtanmai nooluBelum ada peringkat
- Depresssion During PregnancyDokumen30 halamanDepresssion During Pregnancytanmai nooluBelum ada peringkat
- A Study On Problems of Old Age Based Upon Articles Appearing in P PDFDokumen96 halamanA Study On Problems of Old Age Based Upon Articles Appearing in P PDFtanmai nooluBelum ada peringkat
- Seminar on Alopecia Types and CausesDokumen90 halamanSeminar on Alopecia Types and Causesluckyswiss7776848Belum ada peringkat
- Menopause Rating ScaleDokumen8 halamanMenopause Rating Scaletanmai nooluBelum ada peringkat
- 13029-Article Text-47609-1-10-20121220 PDFDokumen4 halaman13029-Article Text-47609-1-10-20121220 PDFtanmai nooluBelum ada peringkat
- Pediatric Procedures PLAB 1323/1023 74Dokumen5 halamanPediatric Procedures PLAB 1323/1023 74tanmai nooluBelum ada peringkat
- Medical-Surgical Nursing: An Integrated Approach, 2E: Nursing Care of The Client: Integumentary SystemDokumen36 halamanMedical-Surgical Nursing: An Integrated Approach, 2E: Nursing Care of The Client: Integumentary Systemtanmai nooluBelum ada peringkat
- Maternal IsoimmunisationDokumen47 halamanMaternal IsoimmunisationDanica Joy Vinluan JacobaBelum ada peringkat
- Bag Technique Lecture Notes PDFDokumen4 halamanBag Technique Lecture Notes PDFtanmai nooluBelum ada peringkat
- Standardized TestDokumen5 halamanStandardized Testtanmai nooluBelum ada peringkat
- Abnormal Uterine Action GuideDokumen27 halamanAbnormal Uterine Action Guidetanmai noolu100% (1)
- 1.modern Concepts of Child CareDokumen18 halaman1.modern Concepts of Child Caretanmai noolu100% (1)
- Seminar On Obg UnitDokumen79 halamanSeminar On Obg Unittanmai noolu100% (2)
- Ante Partum HemorrhageDokumen30 halamanAnte Partum Hemorrhagetanmai nooluBelum ada peringkat
- Care Plan 25 Major Depressive Disorder: Ineffective CopingDokumen11 halamanCare Plan 25 Major Depressive Disorder: Ineffective CopingumaraniBelum ada peringkat
- Care Plan 25 Major Depressive Disorder: Ineffective CopingDokumen11 halamanCare Plan 25 Major Depressive Disorder: Ineffective CopingumaraniBelum ada peringkat
- Essential Seminar on Disaster Nursing RolesDokumen22 halamanEssential Seminar on Disaster Nursing RolesSanvar Mal Soni100% (1)
- Synopsis Proforma For Registration of Subject For DissertationDokumen17 halamanSynopsis Proforma For Registration of Subject For Dissertationtanmai nooluBelum ada peringkat
- Rajiv Gandhi University of Health Sciences Bangalore, Karnataka Annexure - 2 Proforma For Registration of Subjects For DissertationDokumen19 halamanRajiv Gandhi University of Health Sciences Bangalore, Karnataka Annexure - 2 Proforma For Registration of Subjects For Dissertationtanmai nooluBelum ada peringkat
- Burns Management PDFDokumen7 halamanBurns Management PDFRoh Bungaria N Garingging100% (1)
- Class Room Teaching ON MicroteachingDokumen22 halamanClass Room Teaching ON Microteachingsaleha sultana33% (3)
- 11 - Chapter 3 PDFDokumen11 halaman11 - Chapter 3 PDFtanmai nooluBelum ada peringkat
- DR Skills LabDokumen14 halamanDR Skills LabHameda MangulamasBelum ada peringkat
- Sectio CaesareaDokumen13 halamanSectio CaesareaDavid ZamrilBelum ada peringkat
- Octaseeds Rise Review Posttest Compilation 120qDokumen19 halamanOctaseeds Rise Review Posttest Compilation 120qAngela Saldajeno100% (3)
- Resume Obs 21-27 Februari 21Dokumen6 halamanResume Obs 21-27 Februari 21imamsantos1191Belum ada peringkat
- Postterm Pregnancy RisksDokumen13 halamanPostterm Pregnancy RisksArjay AmbaBelum ada peringkat
- The Components of LaborDokumen4 halamanThe Components of LaborMARIANNE JOY ELEAZARBelum ada peringkat
- Handout # 10Dokumen22 halamanHandout # 10Ram August100% (1)
- Case 5Dokumen16 halamanCase 5Angel MayBelum ada peringkat
- Is This Primip A Nullip? The Daily Abuse of Language in ObstetricsDokumen3 halamanIs This Primip A Nullip? The Daily Abuse of Language in ObstetricsuzairBelum ada peringkat
- Narrow Pelvis. Anomalies of Position and Fetal Presentation. Pregnancy and Childbirth During Pelvic Presentation.Dokumen18 halamanNarrow Pelvis. Anomalies of Position and Fetal Presentation. Pregnancy and Childbirth During Pelvic Presentation.mudeyBelum ada peringkat
- Notes On Obstetrics: Normal Labor (Theories of Labor Onset)Dokumen22 halamanNotes On Obstetrics: Normal Labor (Theories of Labor Onset)Jobelle Acena100% (1)
- Delivery Room Case Scenario Activity Sheet: Guide QuestionsDokumen4 halamanDelivery Room Case Scenario Activity Sheet: Guide QuestionsMark VincentBelum ada peringkat
- Mechanism of Labour (Normal and Abnormal)Dokumen27 halamanMechanism of Labour (Normal and Abnormal)Rani100% (1)
- CASE DISCUSSION Subgroup 1 1Dokumen112 halamanCASE DISCUSSION Subgroup 1 1Kartik SharmaBelum ada peringkat
- Fundal HeightDokumen10 halamanFundal HeightASHLEY DAWN BUENAFEBelum ada peringkat
- Breech Presentation - CGDokumen13 halamanBreech Presentation - CGJun MingBelum ada peringkat
- Obstructed LabourDokumen24 halamanObstructed LabourNatukunda Dianah50% (4)
- Intrapartum (Process of Labor Delivery)Dokumen206 halamanIntrapartum (Process of Labor Delivery)coosa liquorsBelum ada peringkat
- Intrapartum Emergencies GuideDokumen34 halamanIntrapartum Emergencies GuideDrChauhanBelum ada peringkat
- Persalinan Sungsang FixDokumen49 halamanPersalinan Sungsang FixElza Nurrifqah100% (1)
- O&G Clerking ScriptDokumen4 halamanO&G Clerking ScriptA VHRSEBelum ada peringkat
- Fetal PositionsDokumen4 halamanFetal PositionsNader Smadi100% (1)
- Seminar On Abnormal Labour and Its ManagementDokumen20 halamanSeminar On Abnormal Labour and Its ManagementPreeti ChouhanBelum ada peringkat
- Face PresentationDokumen4 halamanFace PresentationRose Ann HajironBelum ada peringkat
- High Risk of PregnancyDokumen16 halamanHigh Risk of PregnancyGeraldine PatayanBelum ada peringkat
- Delivery Room Nursing EssentialsDokumen9 halamanDelivery Room Nursing EssentialsTintin HonraBelum ada peringkat
- Maternal Nursing Care - CHPT 12 The Process of Labor and BirthDokumen45 halamanMaternal Nursing Care - CHPT 12 The Process of Labor and Birththubtendrolma100% (6)
- Umbilical Cord ProlapseDokumen26 halamanUmbilical Cord Prolapsesulekhaanoob100% (2)
- OBGYN 2022 + FM 122 PagesDokumen122 halamanOBGYN 2022 + FM 122 PagesDr. zesty anatomistBelum ada peringkat
- N222 Lecture Notes Sp13Dokumen198 halamanN222 Lecture Notes Sp13Jacinth Florido FedelinBelum ada peringkat